
INTRODUCTION
Delirium poses a major challenge to healthy aging, because of its associations with increased mortality,1 higher costs of medical care,2 and increased risk of cognitive impairment and dementia.3–5 Delirium is more common among hospitalized older adults,6,7 and inpatients should be monitored carefully so that risk factors such as pain, sedation, and sleep deprivation, can be mitigated.8–10 Current standard of care for delirium monitoring is by regular bedside assessment,8 e.g. using the Confusion Assessment Method for the ICU (CAM-ICU)11 or the Intensive Care Delirium Screening Checklist (ICDSC).12 Yet bedside assessment is at times hampered by uncertainty about the patient’s premorbid cognitive capabilities, level of training of the assessor, and contemporaneous clinical demands of the nursing staff.13–15 As a result, delirium screening and documentation practices vary widely across institutions: adherence rates as low as 18% and as high as 74% are reported in recent literature.16–19 To address these inconsistencies and improve care of patients with delirium, alternate approaches to delirium screening remain an active area of investigation.20–23
Electroencephalography (EEG) provides an objective measure of dynamic changes in brain activity and can be performed at the bedside in acutely ill patients. Metrics derived from EEG signals show promise as a means of screening patients for delirium based on physiologic changes in the brain.23–31 Although EEG activity patterns change with age and with age-related neurodegenerative diseases such as dementia,32–34 most clinical studies have historically excluded participants over the age of 90 due to low population numbers, leading to concerns for risk of breaches in confidentiality. Very few studies have examined neurophysiologic metrics among individuals over 90 years of age, despite the fact that this segment of the population has grown substantially in recent years, and is projected to more than double in the next 2 decades.35 Furthermore, despite the increased risk of delirium with dementia and the increased risk of dementia with advancing age, the effects of dementia on EEG markers of delirium are largely unknown.36,37
We recently developed an EEG-based metric of delirium (which we refer to in this paper as the EEG Delirium Index, or EEG-DI). EEG-DI is derived from quantitative analysis of the frequency composition, also known as the spectral profile, of raw EEG brain signals, recorded over a five-minute period. In our prior study of EEG-DI measurements over 24-hour recordings in 25 mechanically ventilated adults, EEG-DI ranged between 0 and 3, with higher values observed in patients with normal sensorium (median (IQR) 1.7 [1.6, 2.0]), lower values observed in delirium (1.0 [0.9,1.4]), and the lowest values observed in coma (0.8 [0.6,0.9]).31 Though the EEG-DI showed high discrimination in the derivation cohort (optimism corrected area under the receiver operating curve of 0.94 for distinguishing normal sensorium from delirium and coma), the EEG-DI has not been validated in other populations, including older adults and those with neurodegenerative disease; its generalizability is thus unknown. In the current study, we aim to evaluate the EEG-DI in a retrospective cohort of hospitalized patients 90 years and older (heretofore referred to as nonagenarians). Additionally, we aim to describe the influence of dementia on the performance of the EEG-DI in this cohort.
METHODS
Study Participants
This study was approved by the Vanderbilt University Institutional Review Board (IRB protocol number 201356). We report the findings according to the guidelines set forth by the Standards for Reporting Diagnostic Accuracy Studies (STARD) 2015,38 and the GREENBEAN checklist for reporting studies evaluating the effectiveness of EEG-based biomarkers.39 Participants were identified by a search of the Vanderbilt University Medical Center inpatient EEG database. We screened all EEG recordings from the beginning of the archive of our center’s current EEG recording system (May 25, 2014) to January 31, 2020. We included hospital inpatients aged 90 years or older at the time of recording. If multiple recordings were identified in a single patient, only the first recording during the study period was included, to avoid repeat observer bias. Participants were excluded if the EEG tracing could not be retrieved from archive, if the EEG recording could not be adequately denoised for quantitative analysis (see details of denoising procedures in section 2.4 below), or if delirium could not be unequivocally determined from chart review. Although the final data analysis was not completed until July 2025, we avoided extending the data collection period to limit potential impacts of changes in our hospital practices during the COVID-19 pandemic.
Clinical Data Extraction
The clinical and demographic history was obtained by two coauthors (SC, SWR) who independently reviewed the electronic medical record. History of dementia (dichotomous) was determined by review of admission and discharge records. We considered the level of detail provided in inpatient charts insufficient to consistently determine type or severity of dementia, thus this information was not collected. Presence of delirium at the time of EEG was determined using a modified protocol of the Chart-Based Delirium Identification Instrument (CHART-DEL), a validated chart review method for detection of delirium among hospitalized patients.40 While the CHART-DEL identifies any delirium during the hospitalization, our protocol focused in on the timeframe within 12 hours of the EEG start time. We excluded patients who had evidence of coma (Richmond Agitation-Sedation Score41 of -4 or -5) at the time of EEG. Our protocol drew data from physician notes, nursing flowsheets documenting neurologic assessment (e.g. using the CAM-ICU), and technician annotations of patient responses to standard stimulation procedures at the time of the EEG recording. In absence of formal delirium screening data, nursing assessments documenting a Glasgow Coma Scale (GCS)42 score less than 1511 were considered positive for delirium only if the level of cognitive function was documented to be worse than prehospital baseline, based on contemporaneous discussion with a knowledgeable surrogate. In two cases, we could not reliably determine whether the patient had returned to their premorbid level of cognitive functioning based on chart abstraction; these cases were excluded from further analysis. All group assignments were performed independently by two authors (SC and SWR) who were unaware of the EEG-DI values at the time of group assignments. No discrepancies were identified.
EEG Recording, Preprocessing, and Signal Analysis
Methods for recording EEGs, denoising and preparing the raw signals for spectral analysis are detailed in Appendix A. During this process, one EEG recording was discarded due to too few data epochs available after artifact removal to produce reliable metrics. For the remaining recordings, and following our previously published algorithm, we used global (across the head) averages of selected band power and spectral variability values to compute the EEG Delirium Index (EEG-DI)31 Briefly, the EEG-DI is a continuous variable derived from a linear combination of global average EEG oscillatory power and spectral variability in defined frequency ranges, according to the following equation:
EEG-DI = log((15·7*SVD) + (1·1*SVB2) + (0·7*RTP) + (1·5*RAP))
where SVD and SVB2 indicate spectral variability (coefficient of variation in oscillatory power) in the delta (1-4Hz) and high beta (25-40Hz) frequency ranges, respectively, while RTP and RAP indicate relative spectral power (ratios normalized to broadband 1-40Hz power) in the theta (4-8Hz) and alpha (8-13Hz) frequency ranges, respectively. In our prior work, these frequency-based metrics were identified using a data-driven, penalized variable selection process to optimize information contributing to the EEG detection of delirium or coma. We computed their values using Chronux,43 a MATLAB®-based toolbox, augmented by a series of bespoke MATLAB® functions.
EEG preprocessing, artifact removal and spectral analysis computations were conducted by one coauthor (JN) with process verification by another coauthor (SWR). Because the computations were not subject to interpretation, these coauthors were not blinded to the clinical data at the time of EEG-DI computation and verification.
Statistical Analysis
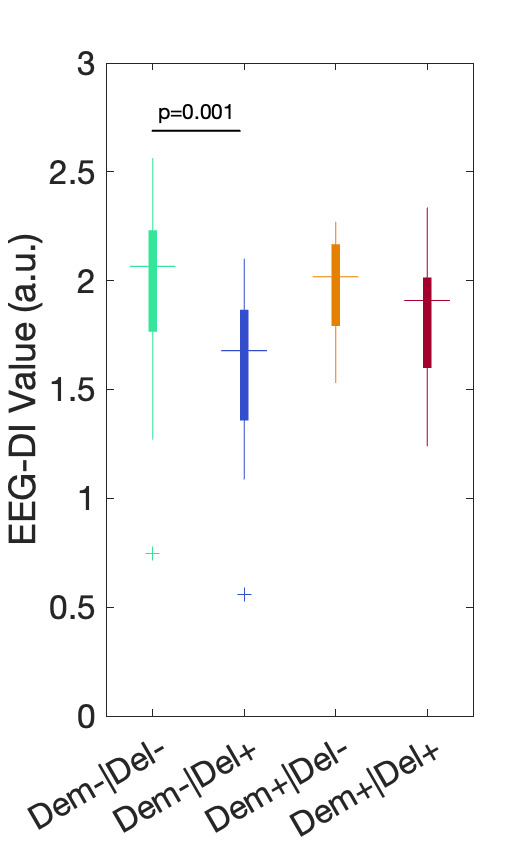
We use descriptive statistics with means and standard deviations or quartiles, as appropriate, to characterize the dataset. We graphically depict the medians and distributions of all metrics, grouped based on history of dementia and presence of delirium. To limit the risk of spurious findings associated with multiple comparisons, and because the primary focus of the current analysis regards the EEG-DI, we excluded formal statistical comparisons of metrics other than the EEG-DI, and examined their distributions for descriptive purposes only.
To estimate the independent effect of delirium associated with a 1-point decrease in EEG-DI among the entire cohort, we built a multivariable logistic regression model adjusting for the following covariates: age, sex assigned at birth, presence of sedatives during EEG, and history of dementia. To further examine the performance of EEG-DI as a screening tool for delirium in participants with and without dementia, we divided the cohort into subgroups by dementia history, and computed the optimism-corrected area under the receiver operating characteristic curve (ROC), along with its 95% confidence interval, for each subgroup. Internal validation was accomplished by bootstrapping as detailed in Appendix B. To estimate the diagnostic accuracy of EEG-DI in the current sample, we computed Youden’s J index,44 and report information-based psychometric properties (sensitivity, specificity, positive and negative predictive values, and positive and negative likelihood ratios) using the associated EEG-DI value as a threshold. Statistical analyses were prespecified and performed using R version 4.2.2.
RESULTS
Of 10,456 EEG recordings performed at our institution during the study period, 182 were performed on patients 90 years and older. After exclusion of repeat EEGs and of 13 patients meeting other exclusion criteria, 68 participants with EEGs remained for the final analysis (Figure 1). Demographic and clinical characteristics of the final cohort are presented in Table 1. Median and interquartile range (IQR) for age was 92 (91, 94) years, and 42 (62%) were female. The two most common reasons for admission were altered mental status and stroke, both occurring in 15 (22%) of individuals, and the most common reason for EEG was altered mental status in 26 (38%), followed by seizure-like activity in 20 (29%). History of dementia was reported in 22 (32%) cases, and 32 (47%) were classified as having delirium. Of the 9 patients receiving sedatives within 12 hours of EEG start time, 1 was on continuous dexmedetomidine infusion, 2 were on continuous propofol infusions, 2 were on continuous lorazepam infusions, and 4 had received one-time doses of lorazepam or clonazepam within 12 hours of EEG.

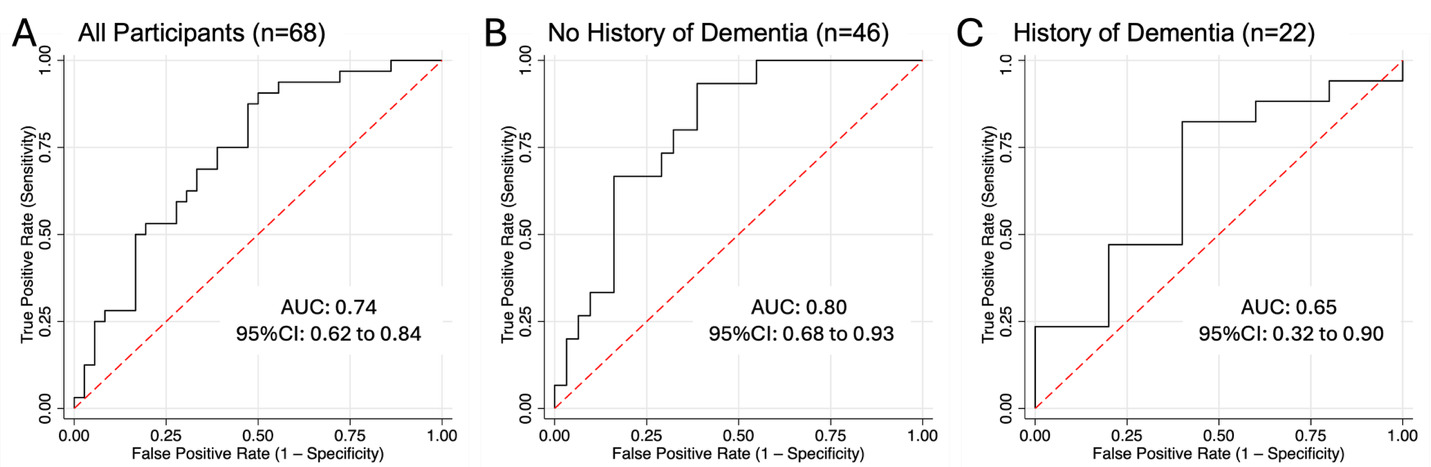
The median value for the EEG-based delirium indicator (EEG-DI) was 1.7 (IQR 1.4, 2.0) among nonagenarians with delirium and 2.0 (IQR 1.8, 2.2) among those without delirium. Subgroup distributions are depicted in Figure 2 for the EEG-DI, and in Supplementary Figure S1 for its component spectral and variability metrics. Controlling for age, sex assigned at birth, sedation and reported history of dementia, a one-point decrease in EEG-DI was independently associated with greater odds of delirium (aOR 11.2, 95% CI 2.0-62.4 p=0.006), meaning a person with EEG-DI of 1.5 was 11 times more likely to have delirium than a person with EEG-DI of 2.5. The receiver operating characteristic (ROC) curves evaluating the accuracy of the EEG-DI as a screening tool for delirium are provided in Figure 3. The optimism-corrected area under the ROC (AUC) was 0.74 (95% CI 0.62 to 0.84) across the entire cohort. In the subgroup analysis, the AUC was 0.80 (95% CI 0.68 to 0.93) among nonagenarians without history of dementia, and 0.65 (95% CI 0.32 to 0.90) among those with history of dementia.
__by_history_of_dementia_and_presence_absence_o.png)
_curve_for_the_eeg-di_as_a_screening_tool_among_hosp.png)
The Youden index was 0.41 at an EEG-DI value of 2.0. In the full cohort, EEG-DI demonstrated high (91%) sensitivity and low (50%) specificity at this threshold. Table 2 details the psychometric properties at this threshold in the subgroups with and without history of dementia, respectively.
DISCUSSION
To our knowledge, this is the largest study reported to date of EEG brain oscillatory patterns in individuals 90 years of age and older. Our previously published EEG-based index (EEG-DI)31 is independently associated with presence of delirium in this cohort, and has the greatest predictive accuracy among participants without known history of dementia. These findings suggest that changes in brain activity patterns associated with delirium among nonagenarians without dementia are similar to younger populations. EEG-based biomarkers of delirium may need to be developed and validated separately for patients with underlying dementia (i.e. delirium superimposed on dementia), who may exhibit unique physiologic patterns of brain activity.
Very few studies have reported EEG findings in nonagenarians. Data from the 90+ Study in a series of 12 cognitively and physically healthy nonagenarians found a high burden of EEG abnormalities (83%), including delta activity in the temporal regions and posterior alpha rhythm slowing.45 These are likely due to acquired “microinsults”, such as subclinical emboli and white matter atrophy, that accumulate in the brain with time and may underlie the increased risk of delirium with age.46 Fractal dimension, a measure of EEG signal complexity, rises during young adulthood and falls after about age 50.37 Complexity measures were not required to compute the EEG-DI; it is possible that their inclusion could improve discrimination of delirium in populations with history of dementia.
We saw weak discrimination of the EEG-DI as a marker of delirium in the subset of patients with dementia, with a distribution of EEG-DI values among the subgroup with delirium and dementia that was largely similar to the distribution among those with neither disorder. Importantly, the subgroup with dementia included only 22 patients, yielding wide confidence intervals for the EEG-DI performance metrics, from worse than chance to excellent performance. The relationship between EEG-DI and delirium among patients with dementia should be assessed in larger, prospective studies before strong conclusions can be drawn. If the discrimination of the EEG-DI is indeed found to be weaker in patients with dementia, this may be due to the heavy influence of the coefficient of variation of the raw EEG signal in the delta (1-4Hz) frequency range, a metric which correlated with worse long-term memory performance in a separate cohort of critically ill patients.47 Delta variability was also increased in a small cohort of patients with Lewy Body Dementia (LBD) compared to healthy controls.48 If increased delta variability is a hallmark of chronic neurodegenerative disease, this may explain a weaker performance of the EEG-DI in the subset of participants with history of dementia. Whether delta variability or other EEG oscillatory dynamics may be an early, subtle characteristic of LBD or other Alzheimer’s Disease-related dementias (ADRD) is worth further investigation; validation of this metric in larger prospective cohorts could lead to more precise differential diagnosis of ADRD for individuals with chronic progressive cognitive impairment.
The EEG-DI, like many other quantitative EEG metrics in the literature, is computed based on global averages (averaging metric values across all EEG channels around the head). Delirium monitoring using limited montage EEG recordings (e.g. frontal-only channels)28,29 is more pragmatic from an implementation perspective.24 Yet few prior studies have evaluated the effects of delirium and dementia on region-specific metrics.49,50 Future studies exploring effects of delirium on brain activity in dementia may attain better discrimination by considering regional patterns in addition to global metrics.
Importantly, our study was conducted in a similar institutional context as the original derivation study. To fully assess generalizability of the EEG-DI, this metric should be prospectively evaluated in an independent, external cohort, preferably across multiple centers and in varying clinical contexts.
This study has several limitations. The identification of dementia and of delirium were determined by retrospective chart review of physician, nursing, technician, and rehabilitation therapist notes, and are subject to measurement bias. Patients did not systematically have prehospitalization cognitive assessments and there were no structured interviews on which to anchor our dementia classification. We therefore relied purely on clinical documentation of the treating providers and could not reliably assess the dementia subtype. Additionally, despite our anchoring the ascertainment of delirium to a validated, chart-based instrument (CHART-DEL),40 the retrospective nature of the study, along with the distinctions between our current population and the validation context of the original CHART-DEL, render this an inherently imperfect classification method. The possibility of residual misclassification of delirium and dementia may be especially relevant for the subgroup analyses, wherein even a single misclassification may meaningfully influence the observed results. EEG recordings were completed according to standard clinical techniques, typically at the bedside or in the EEG suite, and did not include audio/video recordings, thus we could not control for environmental stimuli. Nonetheless, the standard ACNS protocol employed by the EEG technicians combined with the standard-of-care use of CAM-ICU or GCS assessments in our nursing units allowed for contemporaneous identification of delirium or coma with high interrater agreement. The small proportion of participants with known history of dementia resulted in a wide confidence interval estimate for the AUC, limiting our ability to effectively assess the EEG-DI as a reliable test statistic among patients with dementia. Despite the strength of the association between EEG-DI and delirium even after adjusting for dementia in our multivariable analysis, the low estimated AUC in this subgroup suggests that delirium may be mechanistically different in dementia. The distinct spectral profiles among dementia patients demonstrated by distributions of EEG spectral characteristics (Figure S1) support this interpretation and suggest that unique EEG metrics (different from those used to build the EEG-DI) may be required to effectively identify delirium among patients with dementia. To mirror the original derivation study for the EEG-DI, we selected EEG segments recorded immediately after stimulation by the EEG technician. Given the fluctuating nature of delirium, there may be differences between EEG-DI performance at these maximally stimulated timepoints compared to random EEG recording timeframes. Also, a subset of patients received sedative agents (propofol, dexmedetomidine, and benzodiazepines) within hours of EEG recording. These agents are associated with drug-specific effects on the EEG spectra (increased activity in the delta, alpha and beta ranges for GABA-agonists; increased spindle-like activity for dexmedetomidine)51 and may have differentially affected EEG-DI computations. We could not model the effect of distinct sedative regimens without overfitting our models, and chose instead to model influence of sedation as a binary variable. The residual confounding due to heterogeneous sedative exposure may have influenced the observed association between EEG-DI and delirium. Future studies should examine the effects of specific sedatives known to influence the EEG frequency content on performance of EEG-based metrics of delirium.
Finally, and importantly, the wide confidence intervals obtained in our models limit precision of the estimated relationship between the EEG-DI and delirium. We carefully chose our covariates to limit the risk of overfitting, and the exclusion of additional precision variables may have left the primary model incompletely specified. An alternative explanation is that of an unmodeled influence (e.g. that of dementia, or of sedative effect) on the relationship between delirium and EEG frequency composition. In the subgroup analyses, the smaller sample size and low event counts contributed to the wider confidence intervals. In view of this, the magnitude of the associations, in particular the subgroup differences, may be sensitive to sampling variability and should be interpreted with caution.
CONCLUSION
Our previously published EEG Delirium Index was associated with presence of delirium in a retrospective cohort of hospitalized nonagenarians. Our strongest findings support the diagnostic potential of the EEG-DI as an adjunct to existing delirium screening tools among nonagenarians without known history of dementia. Our observations further suggest future studies exploring EEG-based biomarkers of delirium may improve precision by distinguishing among populations based on presence or absence of dementia.
ACKNOWLEDGMENTS
The authors would like to thank the investigators and staff of the Critical Illness, Brain dysfunction and Survivorship (CIBS) Center for scientific discussion to improve the clarity and potential impact of this manuscript. We would also like to acknowledge and appreciate the many patients who entrust their care to our institution and allow their deidentified data to be used retrospectively toward the advancement of science and medicine.
AUTHOR CONTRIBUTIONS
Williams Roberson: Conceptualization, Funding acquisition, Project Administration, Investigation, Methodology, Resources, Software, Supervision, Validation, Visualization, Writing - original draft, Writing - review & editing; Fulton: Project Administration, Investigation, Data curation, Software, Visualization, Writing - original draft, Writing - review & editing; Cyr: Investigation, Data curation, Writing - review & editing; Irlmeier: Formal Analysis, Software, Visualization, Writing - original draft, Writing - review & editing; Wilson: Writing - review & editing; Andrews: Writing - review & editing; Maiga: Funding acquisition, Writing - review & editing; Harrison: Funding acquisition, Writing - review & editing; Bastarache: Writing - review & editing; Jackson: Funding acquisition, Writing - review & editing; Patel: Funding acquisition, Writing - review & editing; Ely: Funding acquisition, Writing - review & editing; Chang: Funding acquisition, Methodology, Writing - review & editing; Haas: Conceptualization, Funding acquisition, Resources, Writing - review & editing; Ye: Funding acquisition, Formal Analysis, Validation, Writing - review & editing; Pandharipande: Funding acquisition, Supervision, Writing - review & editing.
Generative AI Statement
None of the work presented in this manuscript was accomplished with the use of generative AI.
ETHICS STATEMENT
This study was approved by the Vanderbilt University Institutional Review Board (IRB protocol number 201356). The IRB granted a waiver of authorization to use protected health information under US federal code 45 CFR 46.104(d)(4).
FUNDING SOURCES
This work was supported in part by the National Institutes of Health (grant numbers K23AG072030, K23GM150110, R01GM120484, R01AG058639, UL1TR000445 and UL1TR002243, RF1AG075341). The funding sources had no role in study design, data collection, analysis, or interpretation of data, writing of the report, or decision to submit for publication.
DECLARATION OF INTERESTS
None of the authors have financial or personal conflicts of interest to be disclosed.
DATA SHARING
Deidentified data for variables described in this study will be shared in aggregate upon email request to the corresponding author (shawniqua.w.roberson@vumc.org), after signing of a data sharing agreement with Vanderbilt University Medical Center and pursuant to all applicable laws and regulations. Analysis code to preprocess EEGs and compute EEG-DI is freely available online at https://github.com/Cognition-Consciousness-Lab.
Corresponding Author
Shawniqua Williams Roberson, M.Eng., M.D., Departments of Neurology and Biomedical Engineering, Vanderbilt University, 1161 21st Avenue South, MCN A-0118, Nashville, TN 37232. Tel: 615-936-0060; Fax: 615-936-0223; Email: shawniqua.w.roberson@vumc.org ORCID: 0000-0003-1331-380X