
Introduction
Hospital-associated delirium is widely prevalent, and risk of postoperative delirium (POD) following cardiac surgery is compounded by cardiopulmonary bypass, advanced age, underlying cognitive impairment, medications, and other acute and chronic conditions.1 Occurring in up to 50% of adults over age 65 years, POD is the most common complication following cardiac surgery.2 The American Geriatrics Society3 states that up to 40% of delirium cases are preventable, indicating substantial opportunity for practice change.
The Clinical Practice Guideline for Postoperative Delirium in Older Adults by the AGS3 states its first recommendation as standardized delirium education that focuses on teaching nurses and other staff to recognize delirium, understand risk factors, and appropriately utilize screening tools. Despite this recommendation, a local 80-bed cardiac specialty hospital had not added POD to standardized education for nursing staff, revealing an evidence-to-practice gap.
Observations from the cardiac specialty hospital align with evidence demonstrating that many nurses have limited knowledge of delirium incidence, risk factors, and screening tools.4–6 Chart audits indicated that delirium screening documentation was underutilized.
Literature Review
A structured literature review of CINAHL and MEDLINE was conducted to identify recent studies examining delirium education for nursing staff in adult acute care settings (see Figure 1). Searches were limited to full-text, peer-reviewed, English-language articles published between 2018 and 2024. Search terms included delirium and education, delirium and training, and delirium and learning. Delirium education in settings other than the adult acute care setting, such as pediatrics, emergency departments, extended care facilities, hospice, and palliative care were excluded. Studies with patients, families, or healthcare students as the learner were also excluded. Articles were initially screened by title and abstract for relevance, followed by full-text review based on inclusion and exclusion criteria. Thirteen studies were included in the final synthesis (see Table 1).

The literature demonstrates that education improves nurses’ knowledge and screening of delirium and promotes appropriate delirium management.7–16 Studies also link education to increased use of nonpharmacologic strategies, earlier provider notification, and reduced use of potentially inappropriate medications.8,16 Knowledge of delirium alone is insufficient to change patient outcomes17; these findings emphasize the importance of combining staff education with broader systems-level approaches to delirium care.
The literature review was limited to evidence primarily from quasi-experimental and quality improvement projects, and none involved staff education in the cardiac surgery setting. This project aimed to bridge that gap by evaluating a delirium education intervention for nursing staff in the postoperative cardiac surgery setting.
Project Purpose
This project’s purpose was to develop an educational program for nursing staff that aligns with the AGS Clinical Practice Guideline for Postoperative Delirium in Older Adults.3
Outcomes
The anticipated outcomes of the project were three-fold. The first outcome was enhancement of nurses’ knowledge of POD, as measured by the Nurses’ Delirium Knowledge Assessment (NDKA18). The second outcome was improvement in nursing documentation of validated delirium assessments. The third outcome was evaluation of the timing of geriatric consultation as a potential indicator of interdisciplinary response to delirium.
Methods
This uncontrolled before-and-after quality improvement project was conducted between December 2024 and April 2025 and is reported using the Standards for Quality Improvement Reporting Excellence (SQUIRE 2.0) guidelines.19
Context
The site for implementation was an 80-bed cardiac specialty hospital and the postoperative cardiac surgery patient population. The target participants for delirium education included approximately 200 critical care and progressive care nurses and other nursing staff employed at the cardiac specialty hospital.
Intervention
A cardiac surgery nurse practitioner, in collaboration with the hospital’s Clinical Nurse Specialist (CNS), developed evidence-based delirium education with input from the organization’s geriatrician and nurse leaders. Educational content included delirium types with emphasis on the identification of hypoactive and mixed delirium, risk factors, prevention strategies, recognition and screening, appropriate management, and guidance for discussion with patients and their families.
Between January and March 2025, education was presented during required competency updates and a voluntary lunch-and-learn session, which included a PowerPoint presentation, video vignettes of patient scenarios, and one-on-one demonstrations of both the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU20) and the Brief Confusion Assessment Method (bCAM21). Interdisciplinary communication of positive delirium screens was emphasized, including provider notification to support prompt geriatric consultation.
To reinforce learning, delirium education was presented during two consecutive team meetings. The first session included key delirium concepts along with review of the CAM-ICU and bCAM. The second session included case studies of recent patients who had experienced delirium.
Delirium screening documentation was incorporated into quality rounds, held weekdays at noon. During rounds, leadership asked each bedside nurse whether their patients had a positive delirium screening.
Education attendance was not formally tracked. Team meetings included both day and night shift staff, whereas the optional lunch-and-learn session and one-on-one CAM-ICU and bCAM demonstrations were primarily offered during daytime hours. Education was implemented as planned; however, participation in each component was not measured.
Study of the Intervention
This project evaluated changes in nurses’ delirium knowledge, frequency of delirium screening documentation, and timing of geriatric consultation.
Measures
Data was collected from pre- and post-education surveys and chart audits.
NDKA
To measure nurses’ delirium knowledge before and after the educational intervention, the Nurses’ Delirium Knowledge Assessment (NDKA) was utilized.18 The pre-education NDKA was completed by over 60 nursing staff. For staff unable to attend in-person education sessions, pre-education NDKAs were distributed and collected, and a recorded version of the educational PowerPoint was provided via email. Both day and night nurses also had opportunities to participate in informal one-on-one CAM-ICU and bCAM demonstrations during their scheduled shifts. Depending on participation timing, the post-education NDKA was completed before or after team meeting education and reinforcement throughout leadership rounds. Only participants with matched pre- and post-intervention NDKA data (n = 17) were included in the analysis.
Permission to use and modify the NDKA was obtained via email from one of the original study’s contributors (D. Wynaden, personal communication, September 14, 2024). Minor modifications were made to improve relevance to the postoperative cardiac surgery population, including removal of one item specific to orthopedic patients and one item related to gender-specific incidence.22–24 The modified NDKA consisted of 26 items, including one multiple-choice question assessing general delirium knowledge followed by agree, disagree, and unsure responses for the remaining items. A total score was computed for all 26 items.
Pre- and post-education NDKA questionnaires were scored for all participants. Each of the 26 items was assigned one point. Incorrect answers and questions answered as “unsure” were scored as “0”. Correct answers were given a “1”.
NDKA Validity/Reliability. With the initial utilization of the NDKA, Hare et al.18 state that content validity was not assessed; however, Aldawood et al.7 performed a pilot study to evaluate the reliability of a modified version of the NDKA and reported an internal consistency reliability of 0.80.
Demographics. Nurses’ age range, sex, hours worked per week, years of healthcare experience, and educational level were recorded.
Screening Documentation
The organization’s electronic health record (EHR) included an optional delirium screening section based on the four features of delirium (acute change or fluctuation, inattention, altered level of consciousness, and disorganized thinking) in the CAM framework.25 Nurses documented the presence or absence of these features to generate a positive or negative delirium screen. The EHR was structured based on the CAM-ICU for non-verbal patients and the bCAM for verbal patients but did not specify which assessment should be performed; therefore, documentation outcomes were analyzed collectively. Because the organization utilized a universal bed model, intensive care and progressive care patients were analyzed together.
In a meta-analysis, the CAM-ICU demonstrated a pooled sensitivity of 80.0%, and a pooled specificity of 95.9%.26 While the bCAM was originally created for the emergency department, it has been utilized effectively in non-critically ill patients.27 Validity testing of the bCAM in the emergency department setting has indicated a 93% specificity and 65% sensitivity.28
Chart Audits
A chart audit tool was created to track delirium screening documentation and the timing of geriatrician consults. The tool included patient age, delirium screening documentation in the first seven postoperative days, whether delirium was identified during hospitalization, and the postoperative day of the geriatrician consult.
Patient identifiers were not included on the tool. Chart audits were performed on all patients over the age of 65 years who underwent sternotomy with cardiopulmonary bypass in the full month prior to education, December 2024, and in the full month following education, April 2025. The pre-education group included 49 patients, and the post-education group included 42 patients.
Regardless of the number of delirium screenings performed per shift, documentation by the day shift nurse and the night shift nurse was counted once per shift. Documentation was reviewed for up to the first seven postoperative days or until hospital discharge, whichever occurred first. The denominator for each patient consisted of the total number of eligible nursing shifts during hospitalization, and the numerator consisted of the number of shifts with documented delirium screening. The proportion of nursing shifts with delirium screening documentation was calculated for each patient. Timing of geriatric consultation was defined as postoperative day (POD) of the first documented geriatrician consultation. Data from the chart audit tool was converted to an Excel spreadsheet for analysis.
Analysis
Statistical significance was set at p < .05. Intellectus Statistics Software (2024) was used to evaluate the stated outcomes of the intervention with assistance from a statistician.
A Shapiro–Wilk test was used to assess normality of continuous variables. Paired pre- and post-education NDKA scores were analyzed using a two-tailed paired t test. When normality assumptions were met, differences in before and after education delirium screening documentation frequency were evaluated using independent samples t tests. A Mann–Whitney U test was utilized for non-normally distributed night-shift documentation data. Timing of geriatric consultation before and after education was also analyzed using an independent samples t test.
Effect sizes were calculated using Cohen’s d. Power analysis was performed to determine the minimum sample sizes to yield a statistical power of at least 0.80 for detecting small (d = 0.2), medium (d = 0.5), and large (d =0.8) effect sizes, respectively.
Ethical Considerations
Prior to the intervention, approval was obtained from two Institutional Review Boards (IRBs). Nurse participation was voluntary, and the purpose and procedures of the project were explained prior to participation. In accordance with the requirements of one IRB, written informed consent was obtained from nursing staff participants.
Results
Nurses’ Knowledge
Seventeen participants completed a Nurses’ Delirium Knowledge Assessment (NDKA) questionnaire both before and after education.
Demographics
Most of the participants were female (64.71%), bachelor-prepared (70.59%), and had worked in healthcare for 6-12 years (47.06%). Additional demographic details are presented in Table 2.
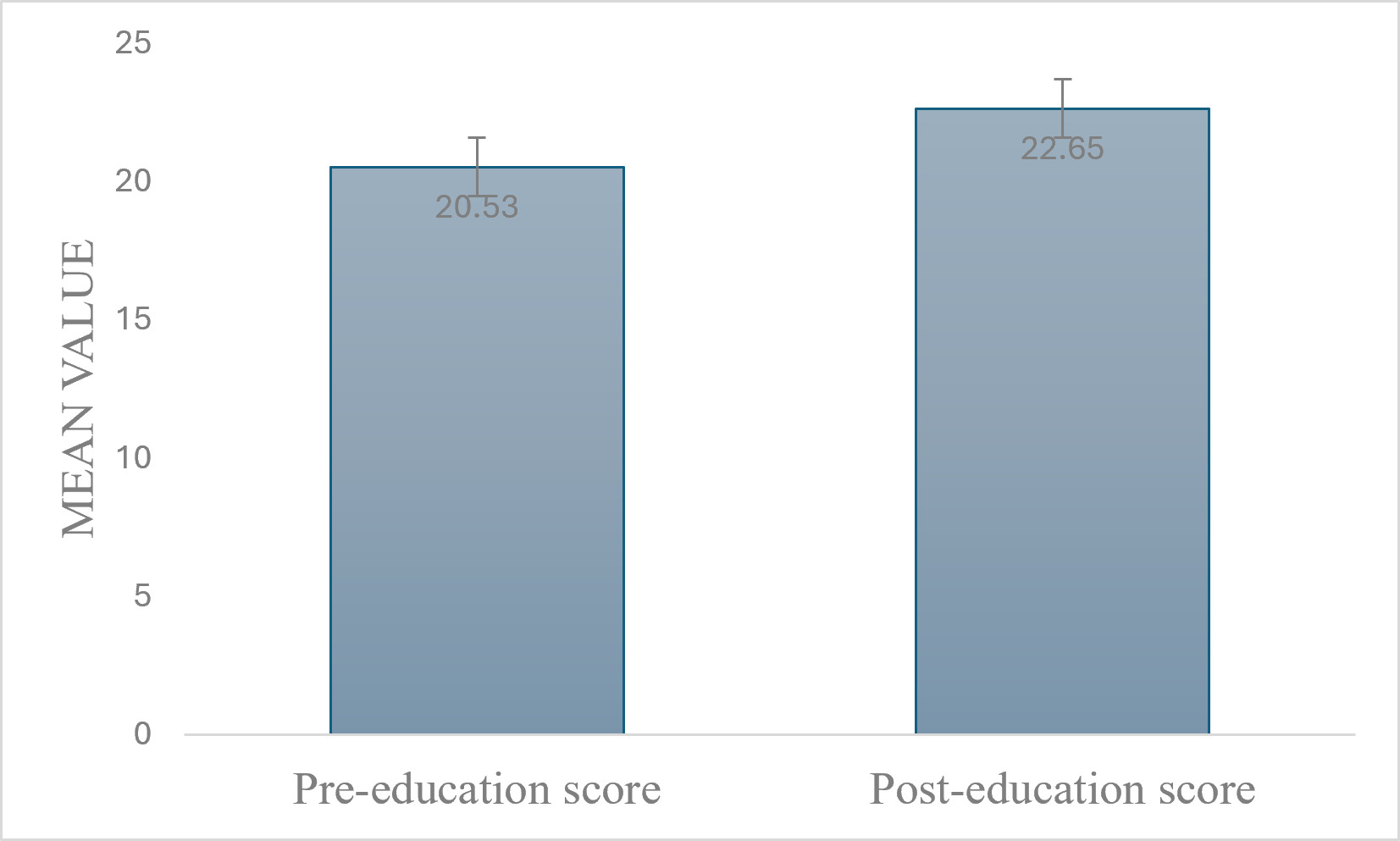
Responses
Pre- and post-education scores were paired using a unique identifier. Based on a total possible score of 26 points, the mean pre-test score was 20.53 (SD = 2.53) compared with 22.65 (SD = 1.93) post-test, indicating a statistically significant improvement [t(16) = -3.65, p = .002] with a large effect size (d=0.884; Figure 2).

Delirium Screening Documentation
Documentation was analyzed separately for day and night shifts, as well as for both shifts combined.
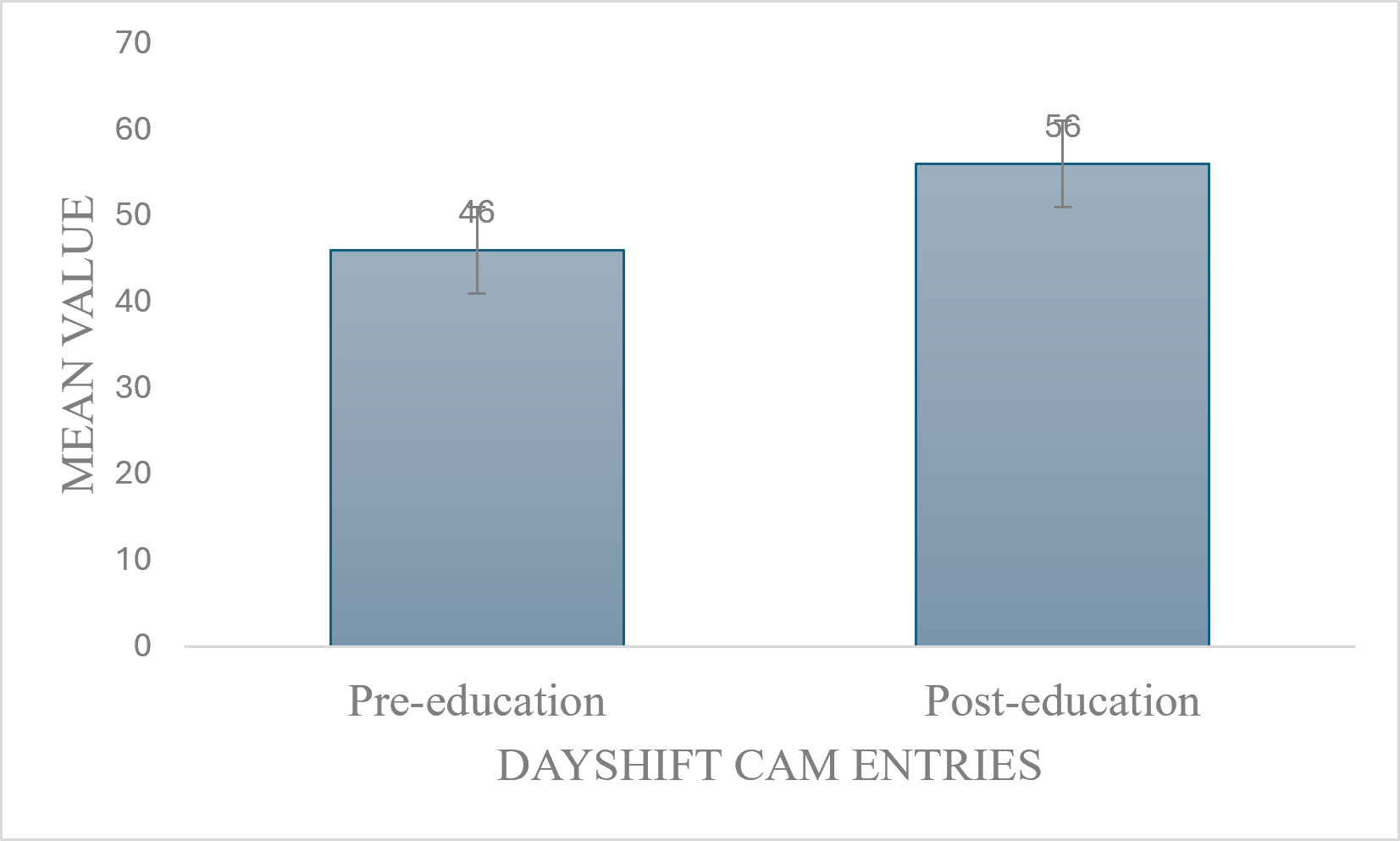
Day Shift
In the pre-education group (n = 49), the rate of completion for day shift documentation was 46% (SD = 0.22) compared with 56% (SD = 0.22) post-education. This difference was statistically significant [t(89) = 2.05, p = .044] with a moderate effect size (d = 0.43; Figure 3).

Combined Shifts
Combined shift documentation did not differ significantly before and after education [t(89) = -0.63, p = .527; d = 0.133].
Night Shift
Night shift documentation was analyzed using a Mann–Whitney U test, with no significant difference between pre- and post-education ranks (U = 1163.5, z = -1.07, p = .283).
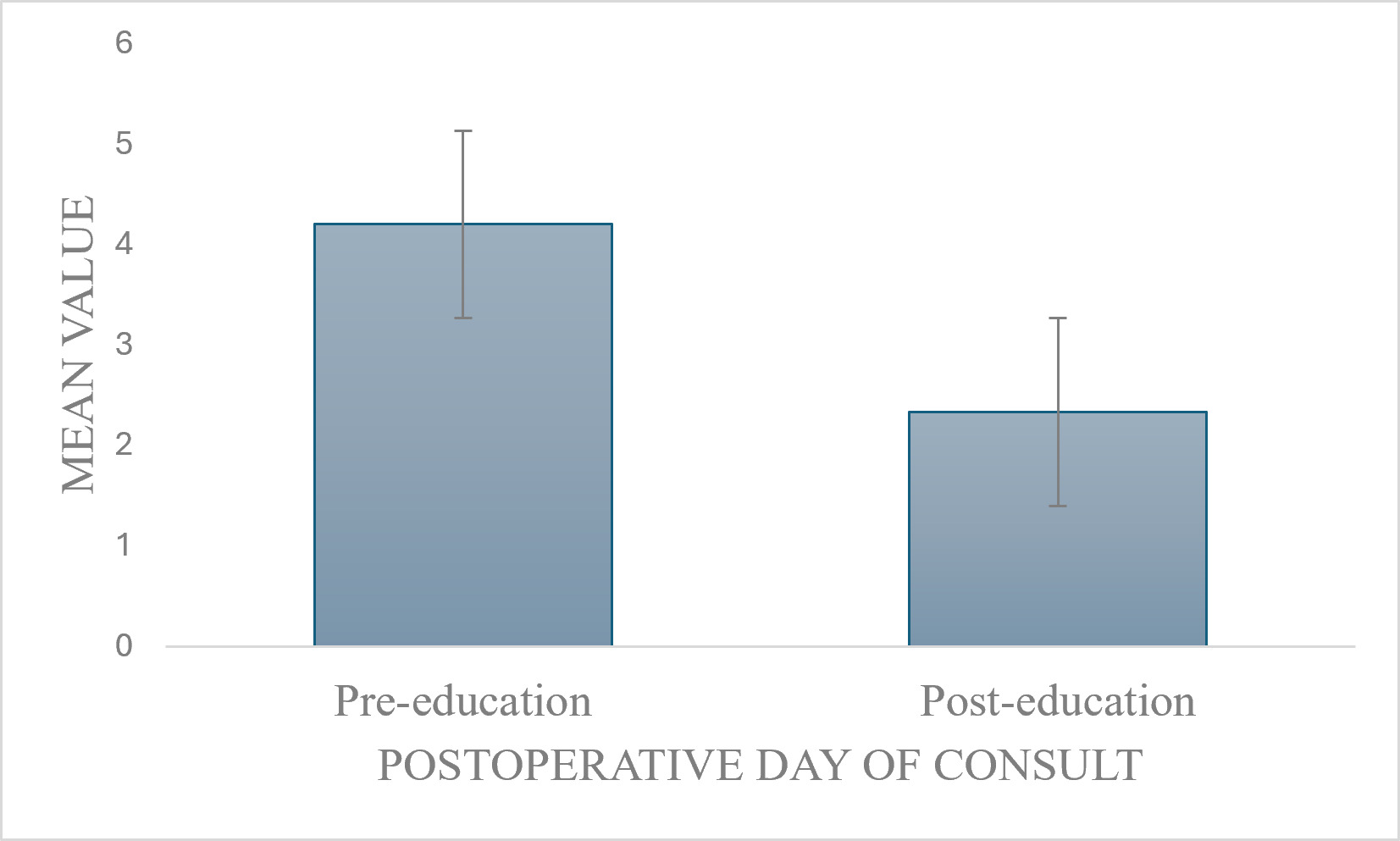
Time to Geriatrician Consult
The mean postoperative day (POD) of geriatric consultation decreased from pre-education (M = 4.20, SD = 3.01) to post-education (M = 2.33, SD = 1.21). Although not statistically significant, the observed effect size was large [t(14) = -1.43, p = .173; d = 0.81; Figure 4].

Discussion
NDKA Responses
The findings are consistent with evidence demonstrating that education improves nurses’ knowledge and awareness of delirium.7–9,11–15 Baseline NDKA scores were relatively high prior to education, indicating pre-existing knowledge of delirium and possibly limiting improvement in scores after education. This may reflect the cardiac surgery population of predominantly older adults, which aligns with previous findings that familiarity with delirium is often higher in geriatric-focused settings29 compared with ICU settings.7 This variation in baseline knowledge may explain the modest improvement observed in this study, despite statistical significance and large effect size.
Over 60 nursing staff completed the pre-intervention assessment; however, post-intervention completion was lower. Because NDKA participation was voluntary, nurses with interest in delirium education or quality improvement may have been more likely to participate, which limits the generalizability of findings.
Delirium Screening Documentation
Improved day shift documentation aligns with literature showing that structured education improves delirium screening practices. Ewens et al.10 reported a significant increase in use of a cognitive assessment tool with documentation rising from 8.5% pre-intervention to 43% post-intervention. Similarly, Travers et al.16 demonstrated improvements in screening rates from 35% to 69%.
Both day and night shift staff received delirium education during required team meetings; however, additional one-on-one CAM-ICU and bCAM demonstrations and an optional lunch-and-learn session were more accessible to day shift nurses. Differences in educational exposure and leadership reinforcement may have contributed to improved day shift documentation. Limited access to education and reduced leadership presence at night have been identified as barriers to consistent implementation of practice change across shifts.30,31 Future educational interventions should include structured strategies to engage off-hour staff.32,33
Geriatric Consult
Although not statistically significant, the trend toward earlier geriatric consultation is consistent with previous research suggesting that education may influence clinical response to delirium. Alhalaiqa et al.8 found that education improved nurses’ ability to detect delirium, while also increasing implementation of nonpharmacologic management and provider notification. Similarly, Travers et al.16 reported practice changes following delirium education, including reduced benzodiazepine use. Together, these studies suggest that improved delirium knowledge may translate into changes in clinical decision-making. In the current project, the decrease in postoperative day of geriatric consultation may reflect increased awareness of delirium and earlier intervention but should be interpreted cautiously due to small sample size (n = 16).
Limitations
The limitations of this project include generalizability, sample size, and instrumentation factors. Because the project was conducted at a single 80-bed cardiac specialty hospital, the results may not be applicable to other hospital settings or patient populations.
The low number of completed pre- and post-education NDKA questionnaires (n = 17) limits interpretation of the intervention’s impact. Because attendance was not formally tracked, staff reach cannot be determined. Pre-intervention survey completion exceeded post-intervention completion, and the overall effect may be underestimated due to the small number of paired responses. Similarly, the small number of patients with delirium who received postoperative geriatric consultation may have contributed to non-significant findings despite a large effect size.
Testing of content validity of the Nurses’ Delirium Knowledge Assessment (NDKA) was not reported by Hare et al.18 Additionally, the NDKA was modified to align with the project setting and target population. While acceptable internal consistency has been reported in modified NDKA instruments,7 the modified version used in this project was not evaluated. These limitations should be considered, particularly given the small sample size.
Nurses’ delirium screening documentation may represent workflow compliance rather than delirium recognition. The impact of increased delirium screening documentation on nursing workload was not evaluated, and compliance may diminish over time without ongoing reinforcement.
Short-term and resource staff were not included in the educational intervention due to organizational structure, and differences in staffing patterns between shifts were not measured, which may have influenced delirium screening documentation outcomes.
Because the EHR did not differentiate between CAM-ICU and bCAM use, delirium screening documentation was analyzed collectively. Findings should be interpreted as documentation practices rather than assessment-specific outcomes.
Sustainability
For project sustainability, delirium education was integrated into orientation curriculum. CAM-ICU and bCAM one-on-one demonstrations were added to annual competency updates to standardize assessment practices. Day and night shift nursing leadership were engaged to reinforce the importance of delirium screening documentation every shift.
Recommendations
Future initiatives should include resource and short-term staff and utilize simulation and case-based learning, as evidence suggests these approaches are more effective than didactic instruction alone (Montgomery et al., 2024). Reinforcement through spaced repetition, case studies, and continued involvement of the geriatric team may further strengthen delirium knowledge and screening practices.9,12
Conclusion
This project highlights that even small, focused delirium educational interventions can improve nursing staff’s knowledge and documentation practices. Future projects should evaluate whether delirium screening documentation translates to changes in care, including non-pharmacologic interventions, medication review, and interdisciplinary collaboration.
Acknowledgements
Derek Trimmer, Nicole Slaten
Author Contributions
Original draft preparation: Dara Commons
Revising and editing: Lori Alesia, Mary Browning, Dara Commons, and Diane Smith
Ethics Statement
Prior to delirium education, approval was obtained by the Ascension St. Vincent and University of Indianapolis Institutional Review Boards (IRBs). Nurses’ participation in the project was voluntary, and project details were fully explained prior to obtaining written informed consent.
Funding Sources
This project did not receive funding from public, commercial, or not-for-profit sources.
Declaration of Interests
There are no conflicts of interest to disclose.
Corresponding author
Conflicts of Interest
None
Funding information
The authors did not receive financial support for the project or its publication.
Abbreviations
American Geriatrics Society (AGS); Brief Confusion Assessment Method (bCAM); Clinical Nurse Specialist (CNS); Confusion Assessment Method (CAM); Confusion Assessment Method for the Intensive Care Unit (CAM-ICU); Nurses’ Delirium Knowledge Assessment (NDKA); postoperative delirium (POD)