Introduction
Most research on delirium is focused on older adults in hospital wards and intensive care units, where delirium is associated with poor health status and caused mainly by acute illness, surgery, or injury.1 Most long-term care (LTC) residents are in a relatively stable condition, or worsen gradually, but they are also at high risk of delirium because of the high prevalence of cognitive impairment (60-70%), functional dependence (50-70%), malnutrition or risk of malnutrition (14% and 53%, respectively), frailty (50%) and prefrailty (40%).2–4 Frailty is almost twice as common in women as in men, noting that women predominate in LTC settings.5 The symptoms of these conditions especially underlying cognitive impairment can also make it challenging to recognize delirium.6
The reported prevalence of delirium in residents in LTC facilities varies widely between countries and settings, ranging from 8.9% in Dutch nursing homes, 14.2% in Belgium, 15% in skilled nurse facilities in the USA, and 18.7% in Spain, to 36.8% in nursing homes in Italy, and even reaching 70.3% in some settings in Canada.7–14 The wide range of reported delirium prevalence supports the NICE guideline recommendation (2023), that a large delirium cohort study be conducted on people residing in LTC facilities.15
Delirium in LTC residents tends to last longer.16 It has the same four fundamental patterns of trajectory as in acute care patients (i.e. improving [fast or slow], worsening, fluctuating, and steady), but LTC residents are at higher risk for worsening compared to patients in acute care setting, due to the higher prevalence of dementia.17,18 A recent large study in LTC across Canada reported that delirium significantly affect residents’ prognosis and their cognitive trajectory at one-year follow-up.19
According to previous studies, despite the high prevalence of delirium among nursing home residents, and validated tools to detect delirium, it continues to go unrecognised at rates of 49%-87% in LTC settings,20,21 particularly in the absence of routine screening with specific assessment tools.22 Staff education, documentation and prevention strategies are important components of a comprehensive approach to delirium assessment in LTC.
Although it is possible to prevent delirium in the hospital setting by providing multicomponent interventions, it is currently unclear if interventions to prevent delirium in LTC are equally effective, and if so which ones should be used.23 A Cochrane review and its update, conducted in 2014 and 2019 respectively, found limited evidence on effective delirium prevention interventions in LTC settings,24,25 Nevertheless, some elements of hospital-based delirium prevention might be translatable to LTC. Health care workers in LTC settings have the advantage of knowing the residents over a long period of time and being able to observe them in their home-like environment in the facility over time. Therefore, a well-trained staff member is more likely to be able to differentiate delirium from dementia and depression. However, research has shown that there is a high staff turnover in LTC, requiring continuous education to maintain a high standard of care.26 It is well known that delirium is under-detected when an objective tool is not formally used or when the health care staff lacks education on this geriatric syndrome.27 Generally, delirium assessment tools are rarely used in nursing homes.27 This might be due to a lack of training of health care personnel and/or time pressures.28
The current gap in the literature, along with the prevalence of delirium in LTC, support the need for recommendations to guide care.
Methods
An extensive search was conducted to identify English language literature from January 2010 until September 2025 on PubMed, MEDLINE, EMBASE, and Web of Science. The search was performed prioritising recent Guidelines, Systematic Reviews and Cochrane Reviews, with primary data searching when no or limited reviews were available. The search query included “delirium” AND “nursing homes” OR “residential facilities” OR “skilled nursing facilities” OR “homes for the aged.” We have limited our search to LTC and in persons age 65 years and older.
Selection criteria for this study included: the use of a validated operational definition or measure of delirium, the reporting of primary data on subjects with delirium, and a focus on the long-term care setting.
Evaluation at the time of admission to long-term care settings
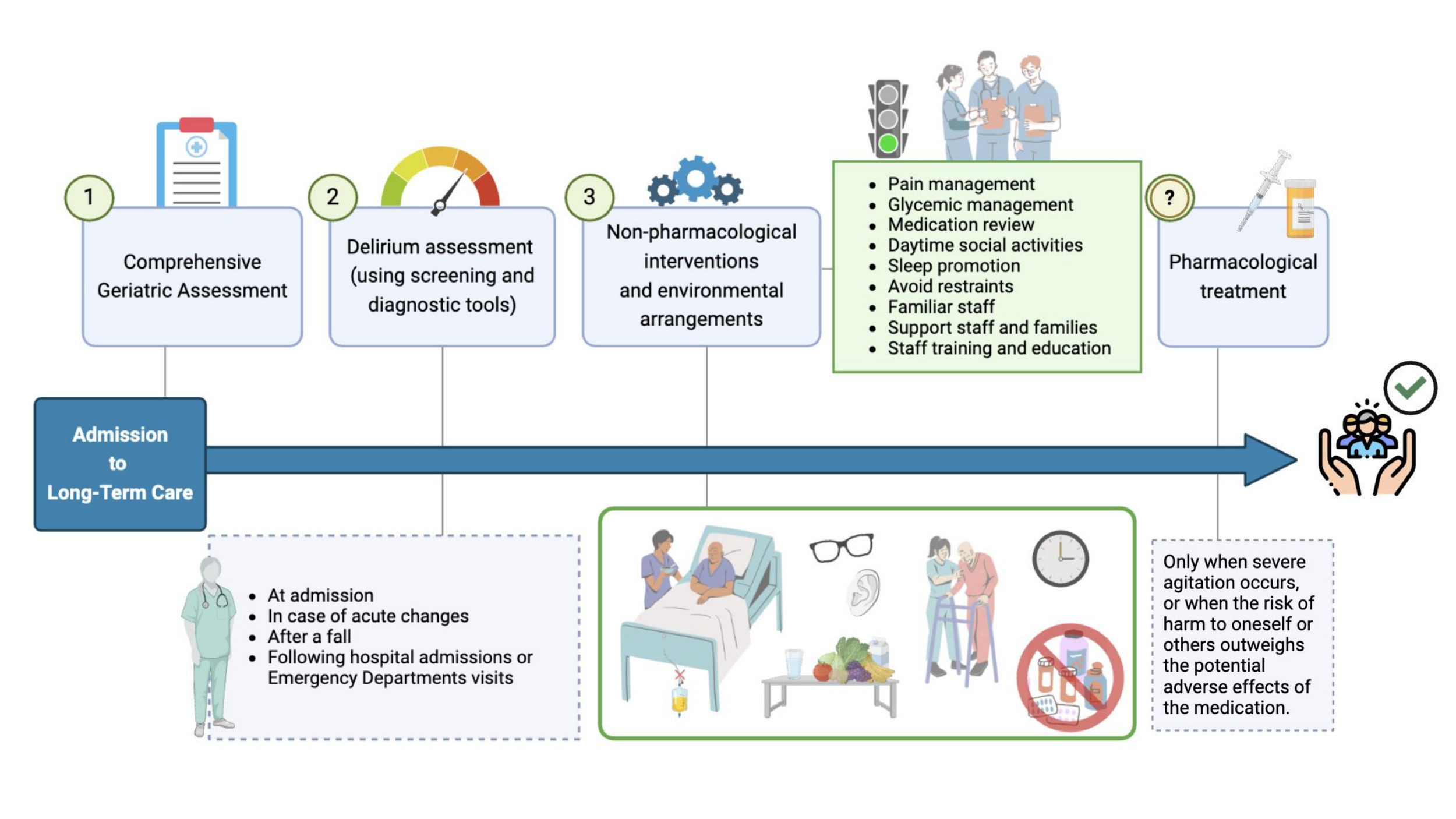
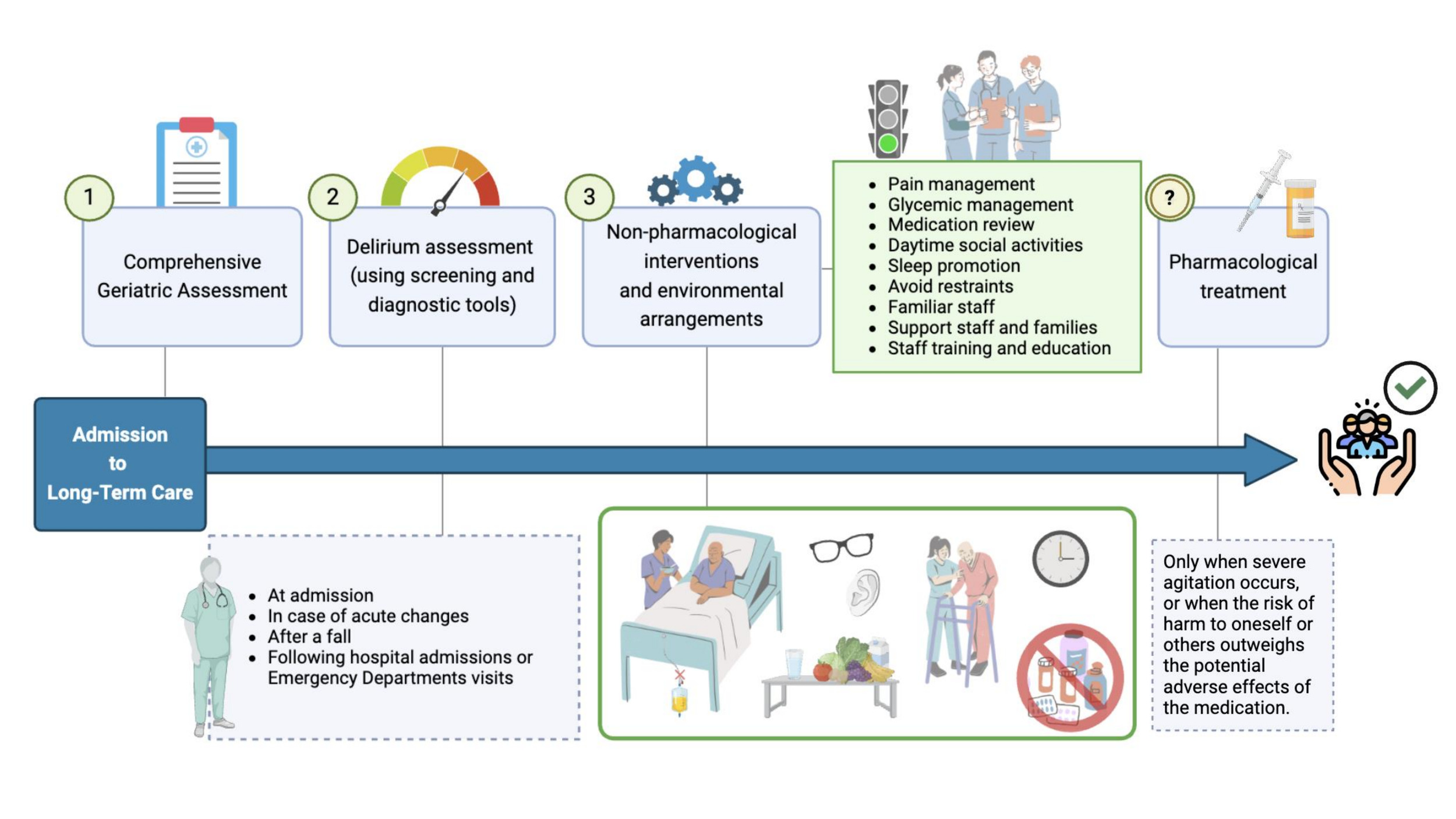
Implication: Every new resident should be assessed, using validated tools, for delirium, cognitive impairment, and depression.9,15 In addition, collateral history and documentation review should seek evidence of any previous formal diagnosis of dementia, and if so diagnosed, any occurrence and the severity of non-cognitive symptoms of dementia (Figure 1).29
Discussion: At the time of LTC admission, assessing the person using a comprehensive geriatric assessment (CGA) is essential.30 CGA usually includes four domains: physical health, functional status, and other parameters such as mobility and quality of life, psychological health (e.g., cognitive and affective status), and socio-environmental parameters (social network, support needs, safety and adequacy). For delirium risk assessment/prevention, key actions are acquiring information on the resident’s cognitive and affective status along with functional status. A recent publication underlines that CGA might reduce the incidence of delirium.30
Delirium and dementia may have some overlapping features and due to lack of knowledge and biases are often unrecognized or mistaken for each other, although they are distinct conditions with separate methods for recognition and different modes of clinical management.13 Screening for delirium helps distinguish delirium from dementia and is supported by the NICE guideline.15 If delirium is detected, best practice recommends that dementia not be diagnosed until delirium is resolved,15 to avoid misdiagnosis. If delirium superimposed on dementia (DSD) is suspected, then that should be the diagnosis rather than dementia alone, because delirium is associated with poor outcomes if not recognized and treated appropriately.31
Different tools can be used for the assessment of cognitive function and depressive symptoms. Functional and motor changes are also supporting features for diagnosing delirium.32–35 It is, therefore, essential to thoroughly evaluate functional status with objective scales at the time of admission. One should be aware that cognitive and functional measures should be reevaluated if the person at the time of LTC admission is diagnosed with delirium since the recorded impairment might not reflect their true baseline status or it might reflect a new baseline, due to the delirium episode.
Screening for delirium
Implication: Each resident should be screened for delirium using a simple and quick-to-administer tool, with a second step evaluation using a validated assessment tool to confirm the presence of delirium where screening is positive.36 The selection of the appropriate delirium screening tool should take into consideration the nurse to resident ratio and the LTC population profile.
Discussion: Delirium screening and detection tools are essential for clinical practice.37 While the evidence supports routine delirium screening in long-term care settings, this is not always possible,15 with staff constraints and limited training being the leading factors. Delirium screening approaches that might be considered include formal tools such as the modified-Richmond Agitation and Sedation Scale (m-RASS), the RADAR (Recognizing Acute Delirium As part of your Routine), the Ultra-Brief CAM (UB-CAM) and the Single Question in Delirium (SQiD). Equally, staff can perform daily observations for indicators of delirium, such as changes in physical function; reduced awareness; increased risk-taking behaviour; being more restless/hyperactive, loud or animated; reduced interest in personal care or in Activities of Daily Living (ADLs); anger / frustration outbursts; decrease in moving around; sleeping more; eating less (Table 1).
Several studies have reported the importance of motor fluctuations for detecting delirium, given that delirium is not an isolated mental disorder but can also affect motor fluctuation.33,34,38–40 The m-RASS might provide key information on motor fluctuations, given its potential to identify motor subtypes of delirium; it has been shown to be highly specific for delirium screening in geriatric and emergency department wards, especially in the context of dementia. Effectiveness of the m-RASS to detect the presence of delirium increases with the number of daily assessments.41,42 Although the m-RASS has not been formally tested in LTC, the evidence of its use in other settings, including patients with dementia, could support future investigation
A nursing tool named RADAR might be helpful in the screening for delirium, especially in detecting the hypoactive subtype with a sensitivity of 73% and a specificity of 67%.43 The RADAR tool includes three questions, which should be answered by the nurses while administering the medications to the patient: 1) was the patient drowsy; 2) did the patient have trouble following your instructions; 3) were the patient’s movements slowed down? The RADAR screening is considered positive when at least one item is “Yes.” The m-RASS and the RADAR can be recorded in the resident’s chart after the daily interaction with the LTC resident.
Another tool which could be considered is the Ultra-Brief Confusion Assessment Method (UB-CAM). The person is first assessed for severe lethargy then asked to tell the day of the week and to repeat all 12 months of the year backwards. If at least one of these two questions are positive it uses a skip pattern to ask additional questions. It takes less about a minute on average, has an accuracy of 89% and has been tested in persons with dementia.44There is also an app available (https://apps.apple.com/us/app/ub-cam-delirium-screen/id1591656740) and a website with free training materials (https://www.ub-cam-delirium-screening.org/).44,45
Family members or volunteers might support healthcare providers with the Single Question in Delirium (SQiD), which involves asking a simple yes/no question, "Do you think [name of patient] has been more confused lately?" This tool has demonstrated good sensitivity and specificity in detecting delirium.46 Engaging family members, particularly in NH settings, may provide valuable support to healthcare providers in the early detection and timely management of delirium. However, this tool should be formally tested in the LTC settings.
The Informant Assessment of Geriatric Delirium (I-AGeD) was developed for lay persons without previous training, as a simple and easily understandable questionnaire to detect delirium in older people. Although initially constructed and validated in a hospital setting, it has been shown to be specific (94%), if not very sensitive (60%) in a LTC setting,47 and might serve as an adjunct to other detection methods.
Regardless of the tool used, data supports the benefit of observing all people in LTC for recent (within hours or days) changes or fluctuations indicating delirium. These may be reported by the person at risk, or a carer or relative. If any of these changes are present the person should have an assessment using an appropriate tool.15 The SQID toll can help formalize this important role of informal carers in delirium detection."
Delirium assessment tools
Implication: Evidence supports the use of the 4AT and Confusion Assessment Method (CAM)-based tools for detecting delirium, even when a dementia is present. (Table 1).36
Discussion: It is important to note the presentation of delirium symptoms in LTC may differ from presentations in hospitals and should be considered on an individual basis. Differentiating delirium from dementia in LTC settings is a clinical challenge due to the significant overlap in their manifest symptoms, such as confusion, agitation, and cognitive impairment. Many delirium cases in LTC are mislabeled as dementia and leads to increased us of psychoactive medications.48 The difficulty is inherently compounded by the high prevalence of baseline dementia among LTC residents; when a patient already experiences chronic cognitive deficits, the acute, fluctuating inattention characteristic of delirium is easily masked or mistakenly seen as the natural progression of their existing disease. Consequently, recognizing a superimposed delirium requires an intimate, historical knowledge of the resident’s unique cognitive baseline, a task frequently complicated by shift changes and staffing constraints, making this vital clinical differentiation both incredibly complex and easily missed. Internationally, research indicates the use of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) criteria49 and the Confusion Assessment Method (CAM) as the approach of choice for delirium diagnosis.50 In various countries, the 4AT and CAM are used for delirium assessment with varying observational tools (Table 1), including the RADAR, Delirium O – Meter.47,51–54
Frequency of delirium assessment
Implication: Early delirium detection in residents is vital to prevent adverse outcomes. Delirium assessment should be completed
-
At the time of admission to the LTC
-
When there is an acute change in mental status or physical function
-
After a fall (unless falls are chronic and recurrent, and concomitant delirium has been ruled out) or if fall frequency increases
-
Upon return to the LTC following an Emergency Department visit or hospital admission
Discussion: Early delirium screening and detection facilitates timely intervention, optimal management approaches and treatment outcomes for older people in LTC. Delirium continues to be under-recognised in this population as many of its presenting symptoms can overlap with other conditions that are common in older people such as dementia, depression or other chronic conditions.16,47 Symptoms of aforementioned conditions can present as subtle and overlapping, making it challenging to differentiate delirium.
Delirium needs to be considered whenever there is a medical illness or a change in vital signs or in the National Early Warning Score (NEWS).55 It is essential that LTC staff are aware of the impact of infection, medicines increasing risk of delirium, reduced activities of daily living, immobility, sensory impairment, urinary catheterisation, urea and electrolyte imbalance, constipation, pain, malnutrition and environmental change on an older person’s risk of delirium.
Regular and systematic assessment might allow for early intervention and management whilst mitigating the negative symptoms of delirium. Longitudinal delirium assessments track a resident’s cognitive status over time to detect any changes that may indicate delirium. In LTC it is imperative, as residents often have multiple risk factors that make them susceptible to delirium, which include advancing age, comorbidities, cognitive impairment, and polypharmacy, amongst others.56 According to Woodhouse et al., longitudinal assessment of delirium in LTC is crucial to achieving high-quality person-centred care.25 However, the limited literature means that research into the requirements of staff in LTC for the assessment and management of delirium requires attention. Further research is needed to identify the optimal implementation of rapid delirium screening tools within the daily workflow of nurses and nursing assistants. Integrating these tools directly into routine practice is critical to leverage the frontline staff’s most valuable asset: their intimate, day-to-day knowledge of each resident’s cognitive baseline, and their frequent contact with the resident across several hours each day.
Non-pharmacological interventions targeting the precipitating factors of delirium
Implication: Non-pharmacological interventions target the important and often multiple precipitating factors for delirium and usually incorporate a multicomponent approach, including15,57:
-
actively look for and treat infection but avoiding overtreatment of urinary tract infection;
-
avoid unnecessary urinary catheterization;
-
review medication to identify medicines associated with increased risk of delirium;
-
assess for pain and initiate treatment where appropriate;
-
address sensory impairment by providing visual and hearing aids;
-
assess and encourage physical activities;
-
address and maintain nutrition and hydration;
-
assess for and address fecal impaction and constipation
Discussion There are various risk factors for delirium, which can be divided into: predisposing factors and precipitating factors (Table 2).21,58 Many of the reported risk factors for delirium are similar in both hospitalised people and LTC residents.8,59,60 Therefore, non-pharmacological interventions, targeting these risk factors, that are effective in hospitals may also have a role in reducing the incidence of delirium in LTC,61 with appropriate modification to account for differences in environmental factors and care processes (McCusker 2013).60
A Cochrane review concluded there were too few studies of interventions to prevent delirium in LTC to identify effective procedures.25 They found only three non-pharmacological interventions aiming at preventing delirium:
-
Providing hydration according to older persons’ needs. This may reduce the incidence of delirium but the effect size was not significant due to methodological limitations.
-
Implementation of a computerized programme that searched for medications that increase the risk of delirium. This probably helped prevent delirium but had no influence on hospitalization and mortality.
-
An enhanced education intervention, which provided learning sessions to the care home staff. This pilot study did not deliver robust conclusions because of the small sample size.
Therefore, NICE proposed a large cohort study be conducted on residents in LTC to determine what impact delirium may have on risk of death, dementia, hospitalization, falls, and other adverse outcomes.15 Such a study should consider multivariable analysis to establish potential significant risk factors and confounding factors and involve cost-effectiveness analyses to select the most efficient preventive measures.15 Although this guideline was updated in 2023, this recommendation for LTC remained unchanged since 2010.
Non-pharmacological interventions for delirium in the LTC should reasonably focus on activities with the most evidence and which are feasible for this setting, including regular hydration, bowel management, mobility, decreasing and avoiding medications causing risk of delirium (Table 3), preventing infection, and behavior strategies that focus on getting to know the older adult. Specifically, residents in the LCT facilities should be encouraged to walk daily whenever feasible. Special consideration should also be given to routine pain assessment, due to the high prevalence of dementia in these settings. For persons with advanced dementia or those unable to express their pain verbally, tools like the Pain Assessment in Advanced Dementia (PAINAD) scale are crucial.62 The PAINAD scale evaluates pain based on five observable behaviors: breathing patterns, negative vocalizations, facial expressions, body language, and consolability. This tool provides caregivers and clinicians with a standardized method to assess and manage pain in nonverbal patients, reducing the risk of untreated pain and possible subsequent delirium,63or indeed inappropriate analgesia when pain is incorrectly assumed.
Pharmacological risk reduction
Implication: The use of psychotropics and other medicines with increasing risk of delirium including medicines with anticholinergic effects should be limited in vulnerable older adults living in LTC, with a careful consideration of risks and benefits before prescribing (Table 3). When these classes of medications are already prescribed, deprescribing should be done via a stepwise dose reduction, monitoring the resident closely.
Discussion: Many psychotropics are commonly used in LTC, and about 30% of residents receive antipsychotics.64–66 (Table 3) Antipsychotics, benzodiazepines and related drugs, opioids, and anticholinergics, including tricyclic antidepressants, are the most common drug groups associated with an increased risk of delirium.67,68 Antipsychotics also increase the risk of serious cardio- and cerebrovascular adverse events, orthostatic hypotension, QTc prolongation, tachycardia, and metabolic adverse effects, as well as sedation and anticholinergic effects.69 Antidepressants differ in their adverse effect profile, such as hyponatremia (SSRIs), QTc prolongation (SSRIs, TCAs), and anticholinergic effects (TCAs). The use of benzodiazepines in LTC residents carries substantial clinical risks, primarily due to age-related changes in drug metabolism and the high prevalence of baseline frailty in this population.70 Most critically, benzodiazepine use is strongly associated with profound psychomotor impairment, leading to a markedly increased risk of debilitating falls and fractures.71 Older adults may experience paradoxical reactions—such as heightened agitation, anxiety, and restlessness—rather than the intended calming effect, underscoring why these agents are generally discouraged for routine behavioral management in LTC settings.72 These medications frequently cause excessive daytime sedation and cognitive blunting, which can severely exacerbate underlying dementia and act as a primary trigger for acute delirium.73 However, the evidence is mainly based on the general older population and/or post- or perioperative situations but not on older vulnerable adults in LTC, although it is likely that the risks are the same or even higher in the vulnerable older population in LTC, who often have several comorbidities, cognitive decline/dementia, frailty and polypharmacy.
Medication review should be a part of the care process and done regularly, at least every six months for older adults living in LTC.74 Regular comprehensive medication review, including deprescribing, should include considerations of changes in overall health and prognosis and be a part of optimizing medications in older adults in LTC.69 When already prescribed, deprescribing should be done via a stepwise dose reduction, monitoring the resident closely74 Medication review should be conducted by general practitioners in collaboration with geriatricians and pharmacists.75
Pharmacological treatment of delirium
Implication: Nonpharmacological management of delirium is always the first-line treatment. Evidence of pharmacological treatment of delirium is poor in older adults in LTC.72 Pharmacological treatment should be considered as a last resort when other treatment options have not been successful, and antipsychotics only in severe agitation, or when the risk of harm to self or others outweighs the potential risks of medications.14 If antipsychotics are needed, their use should be limited to the shortest possible duration and lowest effective dose.
Discussion: Many of the medicines that are commonly used for the treatment of delirium are the same ones that increase the risk of delirium. There is an evidence gap concerning pharmacotherapy of delirium in vulnerable older adults in LTC, with the limited evidence from studies of post- or perioperative delirium. In these populations, there is weak or no evidence for the benefit of pharmacological treatments of delirium based on systematic review of Sadnolova et al. (Table 4).72 According to previous reviews and meta-analysis, the use of antipsychotics did not shorten the duration of delirium or decrease its severity.73,76,77 However, antipsychotics are still used in about 50% of the patients with delirium across different clinical settings, with limited information from LTC.78
Due to the risks of severe adverse effects and events, guidelines recommend that antipsychotics should be considered as a last resort when other treatment options have not been successful, in severe agitation, or when the risk of harm to self or others outweighs the potential side effects of the medication used.15 If nonpharmacological management or treatments have failed and there is a high risk that the older adult in LTC might harm themselves or others, antipsychotics can be used for a few days for extreme aggression/agitation starting at the lowest clinically appropriate dose and titrating cautiously according to symptoms according NICE.15 In that case, the risks and benefits of a specific drug in a particular patient should be examined, considering the resident’s comorbid diseases, cognitive and mental status and severity of these disorders.15 The goal is to reduce psychotic symptoms, noting that the medications do not affect the underlying neuroinflammation or signaling abnormalities, and their use is not intended for the purposes of sedation. The first line of management should be to understand the underlying behavior (not sedate them or cover up behavior with medications) and first attempt to manage behavior without the use of medications."
Non-pharmacological treatment of delirium
Implication: Given the current paucity of evidence of delirium management in LTC, we suggest that LTC staff follow the recommendations provided for delirium prevention. Additionally, staff should be taught behavior techniques, so that they understand that “all behavior has meaning and is need-based”, consider what behaviors can be tolerated safely, learn how to de-escalate behaviors, and become aware of their own verbal and non-verbal responses.
Discussion: Behavior is a form of communication for persons with dementia or delirium and is often driven by an unmet need, e.g., the resident is in pain, needs to urinate, is afraid, bored or over-stimulated, or misinterpreting stimuli because they have dementia or delirium. However, using the term “agitated” or other non-helpful words like “angry” or “aggressive” often leads to chemical and physician restraints. Consider the meaning behind the words you use and describe the behavior instead. Delirium tool kits and techniques such as DICE (https://diceapproach.com) can be used to support staff with better approaches for managing behaviors without medications.79
Simulated family presence is an effective nonpharmacological intervention to reduce agitation in persons with dementia in nursing homes. A simulated family presence through pre-recorded video messages reduced agitation in these hyperactive, delirious patients in hospital.80
Staff Training and Education
Implication: Assure continuous LTC staff education sessions, along with practical use of screening/observation tools and case discussions, and management support for resources and organisation for implementing delirium prevention. Facilitate smooth communication within LTC staff by using the same tools and terms describing resident’s behaviour and symptoms of delirium. Familiarise the staff members with residents to improve delirium detection.
Discussion: Studies have shown that nursing home staff know little about delirium. Several causes have been identified: the fluctuating nature of delirium and its similarity to dementia,13 lack of required education and poor conceptual understanding of delirium, inadequate use of delirium assessment tools, communication barriers and perception of delirium as a burden, which is associated with inappropriate use of tools for delirium detection.81 The educational interventions that are run in acute hospitals may not be easy to transfer to LTC. Therefore, multicomponent interventions to prevent delirium should be specifically adjusted to LTC environment.
Based on the Consolidated Framework for Implementation Research (CFIR) (https://cfirguide.org/) domains of implementation, integrating delirium screening into the electronic or paper-based resident record, providing initial, booster and annual training to staff on the units, utilizing and rewarding direct care unit delirium champions, and providing feedback to staff on adherence with electronic reports or bulletin boards on the units may be considered.
Many delirium programs are not successful beyond the screening stage, especially if staff are not involved in the co-design of the screening frequency and the education about delirium, and do not have access to the resources, toolkits, and staffing needed to carry out best practices for delirium.57 Staff will become discouraged if they conduct delirium screening and then are not supported for the follow-up for a positive delirium screen. Delirium prevention and treatment should be a whole-community approach in LTC.
Other strategies to engage staff include regular debriefings, delirium and dementia huddles, discussion and staff presentation of cases, peer to peer education on delirium, and identification of delirium champions on each shift and unit. Nursing assistants are an integral part of the team in delirium prevention, detection and management, and studies have shown they can assist in delirium screening, and enjoy being involved in delirium care, in acute care settings.82 When staff co-design and co-present education, they are more likely to take responsibility and sustain positive behaviors.
Family and volunteers are also an important part of the team to enhance physical and cognitive function. Studies have shown that informal caregivers are integral in recognizing and managing delirium and delirium superimposed on dementia.83
Molitor et al, based on a literature review, developed a list of factors that may impact the effectiveness of educational interventions concerning delirium in the LTC.84 These are:
-
management support for nursing home staff in implementation of the educational intervention, in terms of providing resources and organization of work time to enable participation in training;
-
awareness that high rates of cognitive impairments among residents may diminish effects of educational intervention, therefore special attention should be paid to differentiating between delirium and dementia, and to teaching staff that delirium often occurs on top of dementia and thus should be considered before labeling as dementia alone. This is critical especially with a transition or change in condition;
-
familiarity with residents – if nursing home staff do not know the residents they have problems with identification of behavioural changes characteristic for delirium;
-
NH staff participation in intervention development provides them with a sense of pride and increases acceptance and interest in the intervention;
-
practical application of knowledge learned during training sessions increases NH staff’s confidence and self-efficiency in providing care preventing delirium;
-
opportunities to discuss case scenarios shared with NH staff enhances their expertise in delirium prevention;
-
support from experts in delirium prevention and treatment on regular basis (for example, once a month sessions) improves NH staff knowledge;
-
communication among the NH staff members plays crucial role in the prevention, recognition and treatment of delirium – it should be done in a structured way using specific terms (e.g. delirium), tools (scales, forms) to detect behavioral changes and communicate them in the same way.
Conclusions
There are limited studies investigating the epidemiology of delirium, its evolution, and outcomes in LTC. There is also a significant gap in the literature on the effectiveness of programs for delirium prevention and treatment in LTC. Recent guidelines recommend that large cohort studies should be conducted among residents in LTC facilities, to guide clinicians on best practices for delirium identification and management. Acknowledging these limitations, we provide a general review on the current knowledge on delirium screening and management in LTC, and offer some practical considerations for implementation.
Conflict of Interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Acknowledgments
Esther Oh is funded by the R01AG076525 (NIA/NIH), P30AG021334 (NIA/NIH), P30AG073104 (NIA/NIH), Sarah Miller Coulson Human Aging Project. Donna M Fick is funded by R01AG030618 (NIA/NIH).