ABBREVIATIONS
aHR, adjusted hazard ratio
CAM-ICU, Confusion Assessment Method for the Intensive Care Unit
FrAILT, Functional Assessment in Liver Transplantation
ICU, intensive care unit
IQR, interquartile range
LT, liver transplant
MELD, Model for End-stage Liver Disease
NIA, National Institute on Aging
NIDDK, National Institute of Diabetes and Digestive and Kidney Diseases
RASS, Richmond Agitation Sedation Scale
INTRODUCTION
Delirium, an acute change in attention or cognition that usually occurs after major illness or surgery, has been recognized among liver transplant recipients since at least the 1980s.1–3 Studies of delirium in both the general hospitalized patient population and among general surgery patients have highlighted poor outcomes among patients experiencing delirium.4–6 Given that there is no effective treatment for delirium and a large body of evidence that prevention is key, it is critical to understand risk factors – particularly modifiable ones – in high-risk populations. Liver transplant recipients have a high prevalence of risk factors for delirium that have been validated among other hospitalized patients and surgery patients, including history of alcohol use.7–10 However, studies of delirium among liver transplant recipients have, until recently, been limited to highly variable prevalence estimates (10-47%) and the identification of few potential risk factors.3,7–15 It is therefore critical to deepen our understanding of delirium in liver transplant recipients, including a more detailed characterization of delirium presentation, risk factors, and associated outcomes.
Among older adults undergoing major general surgery procedures, delirium is associated with increased hospital length of stay and in-hospital mortality.5 Furthermore, recent studies of kidney transplant recipients have found that those who experience delirium have inferior post-transplant outcomes both during and beyond the initial transplant hospitalization. In kidney transplant recipients, delirium is associated with prolonged length of stay, higher risk of discharge to a rehabilitation facility instead of home, and development of post-transplant dementia.16,17 The negative sequalae of delirium has not been well characterized among liver transplant recipients and initial studies are limited to small populations outside of the United States.10,12,18–20 It is difficult to generalize these results to liver transplant recipients in the United States due to differences in recipient demographics, healthcare system characteristics, and severity of patient illness at time of transplant. For example, differences have been noted in percentage of liver recipients whose underlying disease is related to alcohol use, the short-term outcomes after liver transplantation, and the proportion of liver transplants from living donors and their outcomes.21–23 More recent studies of post-liver transplant delirium conducted in the United States have identified only non-modifiable risk factors for delirium9,13 and have provided a limited characterization of the delirium course, limiting their utility in planning prevention strategies.
Therefore, we sought to (1) characterize the presentation of delirium to improve recognition of delirium by providers and (2) evaluate the association between delirium and in-hospital and post-discharge outcomes for liver transplant recipients.
METHODS
Study population
We identified all liver transplant recipients who had been enrolled at the Johns Hopkins Hospital site of the multicenter Functional Assessment in Liver Transplantation (FrAILT) prospective cohort study. This population was under active study at our institution, had delirium data collected as part of clinical care post-transplant, and approximately half of the participants enrolled in the outpatient setting had a pre-transplant frailty assessment using the Liver Frailty Index. Since prior work has shown that frailty is a potentially modifiable risk factor and that, in kidney transplant recipients, frailty is associated with delirium, this also allowed us to perform a limited assessment of frailty as a risk factor for delirium in liver transplant recipients.24 The work described in this manuscript was a secondary analysis of data collected for the FrAILT study. Frailty is a syndrome characterized by the body’s inability to efficiently respond to chronic and acute stressors. Approximately half of the participants who were enrolled in the outpatient setting had a pre-transplant evaluation of physical frailty using the liver frailty index25 that was available for analysis and were followed through their transplant hospitalization. All transplants occurred between 2016 and 2019. This study was approved by the Johns Hopkins Institutional Review Board (IRB00083294).
Donor and recipient characteristics were collected as a part of the FrAILT study and supplemented with information queried from the Johns Hopkins Hospital electronic medical record system. Donor information included type of donor (donation after brain death, donation after cardiac death, or living donor), age, and race. Recipient information included age at transplant, sex, race, Model for End-Stage Liver Disease (MELD) score at time of transplant, liver disease etiology, history of any pre-transplant hepatic encephalopathy, pre-transplant frailty, and whether the recipient had been admitted to the intensive care unit (ICU) pre-transplant. To ensure that all possible exposures that were considered occurred before the outcome of delirium and our study period was limited to the first two weeks post-transplant, we excluded post-transplant factors from consideration as exposures in this analysis.
Delirium assessment
All clinical assessments of the recipients’ cognitive function during their ICU stay post-transplant were abstracted from the electronic medical record. This information included all Richmond Agitation Sedation Scale (RASS) scores26 and Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) scores27 collected as part of clinical care during the recipients’ ICU stay. At our center, all liver transplant recipients are transferred to the surgical ICU immediately after transplant surgery; hospital protocol states that each surgical ICU patient should receive RASS and CAM-ICU assessments at least once per 12-hour nursing shift for the duration of their ICU stay.
Additionally, some liver transplant recipients included in this study were hospitalized pre-transplant. For those who were admitted to an ICU pre-transplant, their RASS and CAM-ICU assessments pre-transplant were also abstracted from the electronic medical record.
Per CAM-ICU protocol, a RASS score of -4 or -5 was defined as coma and the CAM-ICU assessment was not performed. These recipients had a RASS score recorded and their CAM-ICU assessment for that shift was recorded as “Unable to assess”. For all other recipients, a CAM-ICU assessment was performed. A “positive” CAM-ICU score indicated delirium was present and occurred if a patient demonstrated an acute change or fluctuating course of mental status within the last 24 hours, inattention, and at least one of the following: altered level of consciousness (defined by RASS score) and/or disorganized thinking. Those who screened positive for delirium on the CAM-ICU instrument were divided into motoric subtypes by RASS score; those with a RASS score of 0 to -3 were classified as having hypoactive delirium, while those with a RASS score of +1 to +4 were classified as having hyperactive delirium. Presence of delirium on a particular date was defined as a positive CAM-ICU assessment on that calendar day.
Given frequency of misclassification of patients based on CAM-ICU assessments performed as part of clinical care, we performed quality checks on the CAM-ICU data. This included recoding of Feature 1 (acute change or fluctuating course of mental status) to positive/present if the recipient had any recorded non-zero RASS score in the last 24 hours prior to that assessment. Presence or absence of delirium was recoded, as necessary, if a change in Feature 1 resulted in a change in overall CAM-ICU assessment. This resulted in Feature 1 being reclassified from negative to positive for 714/3017 CAM-ICU assessments.
Statistical analysis
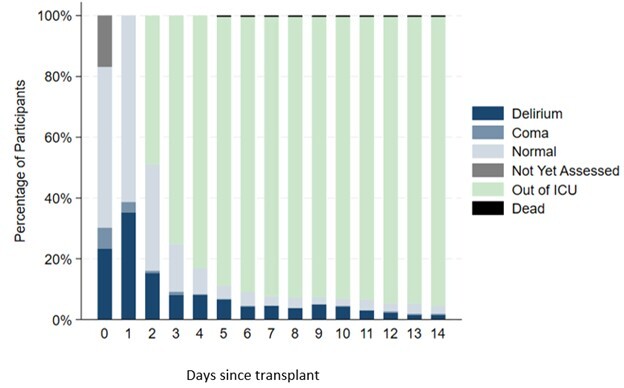
Delirium course was first evaluated using descriptive statistics. This included evaluation of daily status of participants as “delirium” (presence of delirium on at least one assessment), “coma” (presence of coma, or a RASS of -4 to -5, in the absence of a positive delirium assessment that day), “normal” (assessed that day with no evidence of delirium or coma), “not yet assessed” (relevant for post-transplant day 0, if no CAM-ICU assessments were recorded), “out of ICU” (discharged from the ICU to the surgical floor), or “dead”. Status was assessed daily until the first of ICU discharge or post-transplant day 14. Additionally, we assessed cumulative incidence of developing (1) coma or (2) delirium; these were not treated as competing risks in this analysis. For example, a patient who was in a coma based on RASS score could be scored later in their admission as having delirium. Furthermore, we evaluated transitions between statuses (see above) from post-transplant days 0 to 1 and days 1 to 2. This time period was selected based on the results of early descriptive analysis of post-transplant delirium incidence and post-transplant ICU length of stay. Finally, we evaluated the duration of post-transplant delirium as both the number and percentage of ICU days with a positive delirium assessment.
Risk factors for delirium were assessed by comparing recipients who experienced any post-transplant delirium to those who did not experience post-transplant delirium using Chi-square and rank-sum tests for categorical and continuous variables, respectively. Covariates selected a priori (age, sex, MELD score at transplant, history of hepatic encephalopathy, and pre-transplant ICU admission during transplant hospitalization) based on literature review of important variables7–10,13,15 were evaluated as independent risk factors for delirium using multivariable logistic regression. A subgroup analysis among recipients with pre-transplant frailty assessments (N=97) was performed, including presence of frailty as a covariate. Frailty was determined by liver frailty index score of ≥4.5, consistent with prior literature.25
We used Chi-square tests to compare the likelihood of ICU readmission, neurology consult, psychiatry consult, new neurologic or psychiatric diagnosis and/or medications at discharge, discharge location, and hospital readmission at 30 days between these two groups. Neurology or psychiatry consults were at the discretion of the clinical team and can have some overlap. However, in general, a neurology consult would be pursued if a neurologic issue (eg stroke) were thought to be causing altered mental status or other neurologic deficit, while a psychiatry consult would be pursued if the change in mental status was felt to be due to delirium or another psychiatric disorder (eg depression). We used rank-sum testing to compare post-transplant ICU length of stay and hospital length of stay between recipients with versus without post-transplant delirium during their transplant hospitalization. All analyses were performed using Stata 17.1/MP for Windows (College Station, Texas).
RESULTS
Study population characteristics
Of the 261 liver transplant recipients, 42.5% experienced post-transplant delirium. Recipients who experienced post-transplant delirium and those who did not were of similar age [median (interquartile range, IQR) 58 (51-64) vs. 59 (52-65) years, p=0.38], sex (58.6% vs. 64.7% male, p=0.31), race (78.9% vs. 71.3% White, p=0.26), and ethnicity (4.5% vs. 6.7% Hispanic, p=0.46; Table 1). Recipients with and without post-transplant delirium had similar types of donors (87.4% vs. 84.0% donation after brain death, p=0.14). However, recipients who experienced delirium had a higher median (IQR) MELD score at transplant [30 (24-35) vs. 27 (17-29), p<0.001] and were more likely to have a history of hepatic encephalopathy (57.7% vs. 38.7%, p=0.002), have alcohol as the etiology of liver failure (42.3% vs. 26.7%, p=0.03), and be admitted to the ICU pre-transplant (27.0% vs. 7.3%, p<0.001). Among recipients who were admitted to the ICU pre-transplant (N=41), those who experienced delirium post-transplant were more likely to have also experienced delirium pre-transplant (87% vs. 36%, p=0.001).
Characteristics of post-transplant delirium
Recipients’ post-transplant status by day, including presence of delirium or coma, is depicted in Figure 1. Among recipients who experienced delirium post-transplant (N=111), incident delirium occurred on the day of transplant (post-transplant day 0) or the first day post-transplant (post-transplant day 1).
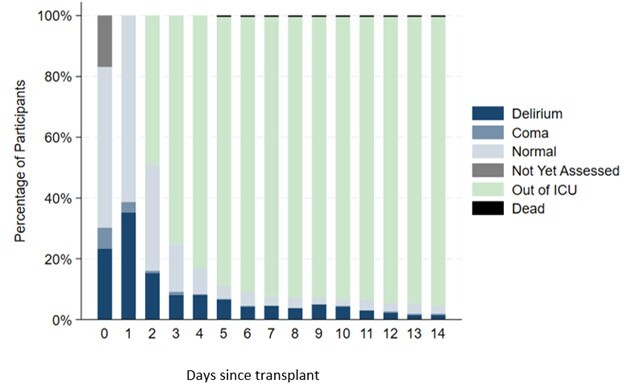
Recipients experienced a transition to delirium from multiple other states. Delirium on post-transplant day 1 was observed among 11% (15/138) of recipients with normal mental status on post-transplant day 0, 72% (44/61) of recipients with delirium on post-transplant day 0, and 61% (11/18) with coma on post-transplant day 0. Of the 44 recipients not assessed on post-transplant day 0, 50% (22/44) had delirium on post-transplant day 1. A transition to delirium on post-transplant day 2 was observed among 22% (2/9) of recipients with coma on post-transplant day 1 but none of the recipients with normal mental status on post-transplant day 1.
Among recipients who developed post-transplant delirium, 58% had hypoactive delirium only, 7% had hyperactive delirium only, and 35% experienced both hypoactive and hyperactive delirium (Table 2). During the first 14 days post-transplant, the median (IQR) duration of ICU delirium was 2 (1, 3) days. This represented a median (IQR) of 50% (33%, 75%) of their days in the ICU during which they had delirium. Among recipients with post-transplant delirium who had a CAM-ICU assessment on the day of transfer out of the ICU (N=94), 30% screened positive for delirium on the day of transfer out of the ICU.
Risk factor assessment for post-transplant delirium
On multivariable analysis, MELD score at time of transplant (aOR 1.06 [95% CI 1.02-1.10] per unit, p=0.001) and pre-transplant admission to the ICU (aOR 2.35 [95% CI 1.02-5.38], p=0.04) were associated with significantly higher odds of post-transplant delirium. Age (aOR 1.01 [95% CI 0.98-1.03] per year, p=0.53), sex (aOR female 1.22 [95% CI 0.71-2.11], p=0.48), and history of hepatic encephalopathy (aOR 1.45 [95% CI 0.83-2.55], p=0.19) were not significantly associated with post-transplant delirium.
Among the 97 recipients who had frailty assessments at transplant evaluation, MELD score (aOR 1.11 [95% CI 1.04-1.18] per unit, p=0.002) was associated with significantly higher odds of post-transplant delirium. Presence of frailty, age, sex, history of hepatic encephalopathy, and pre-transplant ICU stay were not associated with significantly higher odds of delirium.
Hospitalization and post-discharge outcomes
Recipients who experienced post-transplant delirium had a longer median (IQR) ICU length of stay [2 (1-4) vs. 1 (1-2) days, p<0.001] and were more likely to be readmitted to the ICU during their transplant hospitalization (11.7% vs. 4.0%, p=0.02). Recipients with post-transplant delirium were also more likely to have a neurology consult during their transplant hospitalization (18.0% vs. 6.0%, p=0.002) but had similar likelihood of a psychiatry consult (8.1% vs. 4.0%, p=0.25; Table 3). Overall transplant hospitalization length of stay was longer for recipients with versus without post-transplant delirium [26 (13-39) vs. 11 (8-19) days, p<0.001] (Figure 1).
Delirium was associated with lower likelihood of discharge home (64.0% vs. 90.7%) and higher likelihood of discharge to rehabilitation facility (33.3% vs. 6.7%, p<0.001). However, delirium was not associated with 30-day readmission (48.6% vs. 42.0%, p=0.29).
DISCUSSION
In this single-center study of post-liver transplant delirium, we found that incident post-transplant delirium occurred in 42.5% of recipients, began on day 0 or 1 after transplant, and that the most common presentation was hypoactive delirium, which was observed in 58% of recipients who experienced delirium. MELD score at transplant and pre-transplant admission to the ICU were independent risk factors for the development of post-transplant delirium. Frailty was not associated with higher odds of post-transplant delirium. While delirium was only assessed in the ICU, 30% of recipients assessed had delirium on the day of transfer out of the ICU to the surgical floor. Recipients who experienced delirium had a longer ICU length of stay, higher risk of ICU readmission, longer hospital length of stay, and higher likelihood of non-home discharge location.
Some risk factors for delirium identified in this study were similar to risk factors in both the general population and in general surgical populations; however, some were unique.4–6 Older age is a strong risk factor for delirium in other, well-studied populations28 but was not associated with risk of delirium among liver transplant recipients in this study. This might be due to the overall younger age of liver transplant recipients, who nationally have a median age of 50-55 each year.29 Additionally, individuals over age 65 who are listed for and eventually receive a transplant are highly selected to be a relatively healthy and robust group of older patients. This may account for the lack of association between age and delirium observed in our study. Pre-transplant frailty, as measured by the Liver Frailty Index,25 was also not a significant risk factor for post-transplant delirium. While this could be due to limited power secondary to sample size, the point estimates for each group also do not appear clinically different (median 4.4 vs. 4.2 for recipients with vs. without delirium). This differs from findings that frailty is associated with post-transplant delirium in the kidney transplant population,16 although different scales were used to identify frailty in these populations and frailty was not assessed in all the patients within our study population. Additional risk factors for delirium were admission to the ICU pre-transplant, delirium in the ICU pre-transplant, and higher MELD score – an indicator of more severe liver disease. We found a high incidence of delirium among LT recipients who were admitted to the ICU pre-transplant. While pre-transplant delirium assessments were not available in other patients in this study, our group has observed that fewer LT recipients who are not admitted to the ICU have pre-transplant delirium.30 Higher MELD score has been consistently identified as a risk factor for post-transplant delirium among liver transplant recipients in other single-center studies,7,9,10 indicating that severity of liver disease is a key risk factor for this important complication. There might also be some liver transplant recipients who had pre-transplant cognitive impairment independent of their hepatic encephalopathy that was attributed to their liver dysfunction and therefore went unrecognized. Future studies should evaluate this potential risk factor, given its importance in the general population and other surgical populations.
We explored not only the incidence of delirium but also characterized its motoric subtype in liver transplant recipients, finding that a hypoactive (57%) or mixed (37%) motoric subtype was most common. Studies in other critically ill populations have found that delirium frequently goes undiagnosed unless specific diagnostic instruments, such as the CAM-ICU, are being regularly used.31 This is particularly true of hypoactive and mixed motoric subtypes, which are less easily recognized compared to the hyperactive subtypes.32 Therefore, the high frequency of hypoactive and mixed delirium among liver transplant recipients might explain the variable incidences of delirium reported in prior studies.3,7–15 Hypoactive delirium might also contribute to other clinical complications, such as increased risk of aspiration or prolonged immobility. Our finding that delirium occurred on postoperative day 0 or 1 in those recipients who developed it suggests the importance of future work to identify and optimize preoperative and intraoperative factors affecting delirium risk. Additionally, the CAM-ICU assessments used in this study were performed as part of clinical care, not with the intention of being used for research. We noted that feature 1 was incorrectly classified as negative in 23.7% of assessments performed in our study population. This finding underscores the need for rigorous quality control on delirium assessments that are being performed to improve detection of delirium.
Our finding that 30% of liver transplant recipients who experienced post-transplant delirium and were assessed on the day of transfer out of the ICU experienced delirium on the day of transfer also raises the question of whether delirium is common and underrecognized among liver transplant recipients on the surgical floor. This potential under-recognition would be exacerbated by the fact that most of the delirium experienced in this population is the hypoactive motoric subtype. Evaluations of delirium in other populations have noted that involving specialists, such as psychiatrists, in the evaluation of critically ill patients with potential delirium can be helpful.33 Interestingly, we found that, at our center, adult recipients with delirium were more likely than those without delirium to receive a neurology consult but not a psychiatry consult. Therefore, practice patterns at different centers could affect consultant involvement. Further study of post-ICU delirium among liver transplant recipients is warranted to improve prevention, recognition, and support.
It is critical that we understand and address delirium among liver transplant recipients because of its association with inferior outcomes. Our findings of longer ICU length of stay and longer hospital length of stay are consistent with prior studies of delirium in liver transplant recipients,8,9,11–13,15,34,35 though the extent to which this is driven by delirium versus other risk factors that resulted in delirium remains unclear. We noted that 30% of recipients who experienced post-liver transplant delirium in the ICU had delirium on the day of transfer out of the ICU, suggesting that delirium continues to be an issue for many recipients on the floor. We were unable to capture incident delirium on the surgical floor, making our estimates of delirium prevalence likely an underestimate of its true prevalence during the transplant hospitalization. Additionally, we found that delirium was associated with higher risk of ICU readmission and higher risk of being discharged to a location other than home. Similarly, delirium is associated with these inferior outcomes among recipients in studies of kidney transplant recipients.16
Limitations of this study include its single-center design, which might limit generalizability to liver transplant recipients at other centers. However, this study included one of the largest sample sizes to date drawn from a high-volume center performing transplants representing the full spectrum of transplant candidates, used validated delirium screening tools, and had results consistent with prior studies for outcomes that had been previously examined (i.e. hospital and ICU length of stay). An additional limitation of this study is that the CAM-ICU assessments were performed as part of clinical care rather than within a research context, limiting our research team’s control over assessment quality. However, these patients were all admitted to the surgical ICU, which cares for over 130 liver transplant recipients per year. Per protocol, these nurses perform CAM-ICU assessments on all patients, including liver transplant recipients, under their care every shift and have quality checks as part of their nursing management protocols. However, it is well-recognized that some clinical assessments are missed; it is therefore possible that our numbers are an underestimation of delirium among liver transplant recipients despite the high prevalence we observed. Still, we noted that days when only one assessment was performed were more commonly later in a recipient’s ICU stay and that other RASS or CAM-ICU assessments performed that day typically noted a RASS of zero. Combined with the early delirium onset we observed, this hopefully decreases the impact of missed assessments on our findings. Additionally, we noted that Feature 1 of the CAM-ICU score was frequently answered incorrectly based on other documented RASS scores during the relevant time period, which often extended beyond that particular nurse’s shift. Feature 1 errors have been shown to be common and are a source of published quality improvement initiatives.36 However, we recognize that many patients were reclassified based on checks of the CAM-ICU Feature scores, which emphasizes the need for future validation of these results using a prospective cohort in whom CAM-ICU assessments are performed with regular quality checks. Additional intraoperative factors, such as length of surgery, were not assessed in this study and warrant further investigation. Finally, we recognize that these assessments do not replace formal neurologic assessments pre- or post-transplant and that routine clinical assessments of lower quality and consistency than those performed by a specially trained research team.37 We also recognize that, even with formal neurologic assessments, it may be difficult to separate delirium from hepatic encephalopathy, and that it is unclear from current research whether that distinction is meaningful in this population. Still, we feel that this exploratory study of delirium has identified key features of and risk factors for delirium in liver transplant recipients that can inform future work.
In conclusion, post-operative delirium incidence among liver transplant recipients is high and is frequently present on the date of transfer out of the ICU. The predominant hypoactive motoric subtype might cause delirium after ICU transfer to go underrecognized by clinical teams; further study of post-liver transplant delirium prevalence on the surgical floor and sequelae is warranted, particularly given the inferior hospitalization and post-discharge outcomes we observed among liver transplant recipients who experienced delirium. Our findings underscore the frequency and importance of post-liver transplant delirium, as well as the need for further research to explore the efficacy of prevention strategies38 in this population. Delirium prevention and management may be a key element of perioperative care where we can intervene to improve overall outcomes after liver transplant surgery.
ACKNOWLEDGMENTS
We thank Dr. Karen Bandeen-Roche for advice provided regarding the analysis in this manuscript.
AUTHOR CONTRIBUTIONS
Jessica M. Ruck – conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, software, supervision, visualization, writing – original draft, writing – review & editing
Sherif M. Helmy – data curation, project administration, writing – review & editing
Karin Neufeld - conceptualization, methodology, writing – review & editing
Esther S. Oh - conceptualization, methodology, writing – review & editing
Dale M. Needham – conceptualization, methodology, writing – review & editing
Elizabeth Colantuoni – formal analysis, methodology, writing – review & editing
Mara McAdams-DeMarco - project administration, resources, software, writing – review & editing
Jennifer C. Lai – conceptualization, funding acquisition, investigation, methodology, writing – review & editing
Dorry L. Segev – conceptualization, funding acquisition, resources, software, supervision, writing – review & editing
Elizabeth A. King – conceptualization, investigation, methodology, project administration, resources, supervision, writing – review & editing
ETHICS STATEMENT
This study was approved by the Johns Hopkins Institutional Review Board (IRB00083294) and written consent was obtained for all participants. This research was conducted in compliance with the Declaration of Helsinki, and consent was obtained in adherence to the Belmont Report principles.
DATA AVAILABILITY
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
FUNDING SOURCES
This work was supported by grant numbers F32AG067642 (PI: Ruck), K02AG076883 (PI: McAdams DeMarco), K24AG080021 (PI: Lai), and R01AG059183 (PI: Lai) from the National Institute on Aging (NIA) and K24DK101828 (PI: Segev) from the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). The analyses described here are the responsibility of the authors alone and do not necessarily reflect the views or policies of the Department of Health and Human Services, nor does mention of trade names, commercial products or organizations imply endorsement by the U.S. Government.
DECLARATION OF INTERESTS
The authors of this manuscript have no conflicts of interest to disclose as described by Delirium.