Introduction
Delirium is a common and severe neuropsychiatric syndrome characterized by an acute onset of cognitive disturbances that cannot be attributed to a pre-existing or evolving neurocognitive disorder.1–3 Approximately one in four hospitalized adults over 65 experience delirium.4 It is associated with increased mortality, prolonged hospital stay, long-term cognitive decline, institutionalization, and psychological distress, including post-traumatic stress disorder, for both patients and caregivers.1,2,5
Despite the availability of validated screening tools, delirium is frequently unrecognized or misdiagnosed, particularly in its hypoactive form.3 From the patient perspective, episodes may be difficult to articulate, as acknowledging confusion or “losing one’s mind” during hospitalization adds to an already vulnerable situation. Qualitative research describes fear, shame, and difficulties in communication, further complicating diagnoses.6 Nurses, who often conduct initial assessments, report barriers such as time constraints, inadequate training, and limited awareness of baseline cognition. Knowledge gaps are not restricted to nursing staff: medical students also receive inconsistent delirium education and often underestimate its consequences.7
Traditional delirium education mostly consists of face-to-face education, and, to a lesser extent, e-learning and interprofessional education.8 To facilitate the translation from theory to practice, there is growing interest in experiential methods such as virtual reality (VR) simulations,5 which immerse learners in the perspective of patients undergoing cognitive or sensory disruptions.9–11 VR has been shown to facilitate perspective-taking and increase empathy.12–14 Large-scale studies suggest VR simulations lead to more durable behavioral changes than traditional approaches,13 and meta-analytic evidence indicates that VR is particularly effective at enhancing perspective-taking, though effects on empathy are more variable.14 This variability may depend on how VR is implemented, as VR is generally regarded as a highly effective tool for fostering empathy.12,15,16
In clinical education, VR simulations have been used to foster empathic communication and understanding of patient needs.17–21 For example, VR simulations of dementia or sensory loss improved students’ comprehension of cognitive impairment and appreciation of patient perspectives.22 However, delirium has received little attention in VR-based education. A small study with nursing students found VR delirium simulations useful,21 and a quasi-experimental study with 18 nurses showed improvements in empathy and knowledge compared to lecture-based training.23 Yet these studies were limited by small samples and scenarios not explicitly grounded in extended accounts of patient experiences.
With this study, we contribute to the emerging delirium VR research area by evaluating the perceived impact of VR delirium simulations comprising a few key scenes, grounded in qualitative evidence of patients’ delirium experiences24 (which emphasized disorientation, fear, helplessness, and altered perception as main experiences) and input from clinical experts. Through post-simulation survey data, we explored how participants interpreted the simulation’s educational relevance, empathic impact, and potential value for healthcare training.
Methods
Participants and procedure
We recruited 23 university students attending an educational session organized with the Swiss Study Foundation, bringing together university students from diverse disciplinary backgrounds interested in delirium care (as future caregivers) personally or professionally, to deepen their understanding of delirium and to evaluate our immersive VR simulation. Inclusion criteria were age ≥18, German fluency, and no known contraindications to VR (contraindications to VR included a history of epilepsy or severe motion sickness).
Sessions were conducted in a lecture hall configured for parallel VR use, with eleven Meta Quest 3 headsets set up at individual stations to prevent interference. After screening and providing informed consent, participants received a brief orientation, completed a 7-minute VR simulation, and then filled out a 42-item questionnaire on their own devices.
Ethical statement
The study was reviewed using a checklist, according to institutional procedures at the FHNW School of Applied Psychology, and was classified as not requiring cantonal ethics approval (in Switzerland, human subjects research is overseen by cantonal ethics committees). The study adhered to GDPR requirements.
VR simulation
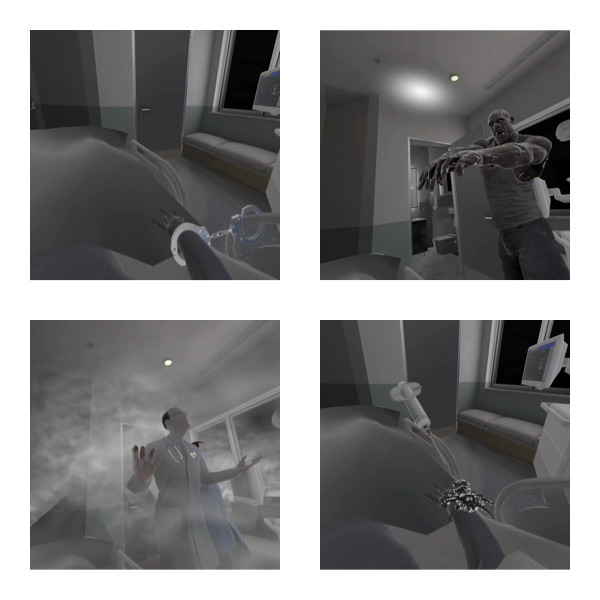
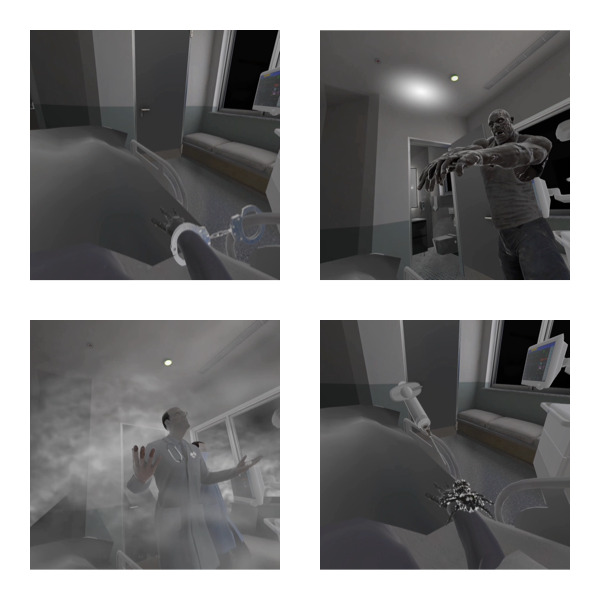
The simulation was developed in Unity and deployed on Meta Quest 3 headsets with integrated audio. Informed by qualitative syntheses of patient experiences24 and clinical expert input, the simulation followed a linear, three-scene hospital narrative (Figure 1): introduction by a nurse; delirium phase with restraint in bed and visual/auditory distortions (e.g., distorted lights, a threatening zombie-like figure, a crawling spider, staff speaking as if the patient were absent); and recovery phase with improved lighting and empathetic staff behavior, underscoring the impact of caregiver interactions.
Measurements
Participants completed a study-specific 42-item questionnaire, covering five domains: usability/immersion, cognitive and clinical learning, emotional engagement/empathy, ethical/public-health considerations, and future directions, plus demographics. Six items adapted the wording of the System Usability Scale25 (SUS); because the full SUS was not administered, no SUS score was computed. While this approach did not allow us to infer validated constructs, it prioritized context relevance and reduced participants’ burden.26 Additional items were conceptually inspired by the User Engagement Scale27 (UES), Immersive Tendencies Questionnaire28 (ITQ), and Toronto Empathy Questionnaire29 (TEQ), but were tailored to VR-based delirium training; accordingly, no UES/ITQ/TEQ scores were calculated. Most items (22) used five-point Likert-type responses, and 7 open-ended questions invited further elaboration after each topic. The open-ended questions were inspired by direct clinical observations as well as the prior work. The full questionnaire can be seen as a Supplementary Material.
Statistical analyses
The Likert items were summarized descriptively. To test departures from the neutral midpoint (3), we ran two-tailed one-sample t-tests with Bonferroni correction across the 22 inferential items (αper-test=0.05/22). While we treated Likert-type responses as approximately continuous for inference,30 we reported Shapiro-Wilk and Wilcoxon signed-rank tests as robustness checks and provided confidence intervals and effect sizes.31To explore response patterns, we computed Spearman inter-item correlations and visualized a correlation matrix; given the adapted nature of our questionnaire, these analyses are exploratory and not intended to validate original scales.
Results
Participant characteristics
The sample consisted of 23 university students (74% aged 18-24; 26% aged 25-34; 56% women). 43% percent reported a medical background; while most did not have professional healthcare experience (52%), 35% had professional healthcare experience and 13% had experience as informal caregivers. Prior exposure to delirium was 48% none, 39% direct, 13% indirect. Regarding VR, 65% were occasional users (21% first-time; 13% frequent). None had previously experienced a delirium-focused VR simulation. Table 1 details the qualifiers used to describe the participants.
Quantitative results (Likert items)
All participants who agreed to join the experiment completed the tasks, i.e., the response rate was 100%, and overall ratings were positive (Table 2). Because Shapiro-Wilk indicated non-normality for most items, Wilcoxon signed-rank tests were reported alongside one-sample t-tests, though that did not change inferences for any item.
Usability and immersion. Participants found the simulation ‘intuitive and easy to navigate’ (M=4.30, SD=0.70, p<.0023), its immersive nature engaging (M=4.22, SD=0.74, p<.0023), and the sensory effects ‘effective in simulating a delirium experience’ (M=4.00, SD=0.67, p<.0023). Items implying negative experiences were near neutrality: about the simulation being ‘cumbersome’ (M=2.30, SD=1.29, p=.017), ‘taxing’ (M=2.65, SD=1.07, p=.134), needing ‘technical support’ (M=2.22, SD=1.13, p=.003), and finding ‘too much inconsistency in the sensory effects’ (M=2.61, SD=0.94, p=.059).
Cognitive and clinical learning. Participants agreed that the VR simulation ‘provided valuable insights into cognitive distortions’ (M=4.22, SD=0.60, p<.0023) and didn’t find it ‘unnecessarily complex’ (M=1.65, SD=0.57, p<.0023). Responses to an improved ‘ability to identify signs of delirium experience’ were above the midpoint but not significant (M=3.61, SD=0.94, p=.005), while responses to an improved ‘ability to differentiate between delirium and dementia’ were neutral (M=3.09, SD=1.02, p=.680).
Emotional engagement and empathy. Participants reported an increase in ‘empathy toward delirium patients’ (M=4.39, SD=0.58, p<.0023) and improved understanding of ‘the emotional distress of delirium patients’ (M=4.13, SD=0.81, p<.0023). They disagreed with ‘viewing the experience of delirium patients in VR did not touch me’ (M=2.00, SD=1.09, p<.0023). Feeling ‘emotionally overwhelmed or anxious during the simulation’ was near neutrality (M=2.61, SD=1.12, p=.107), as well as ‘viewing the experience was too synthetic (game-like) to create empathy’ (M=3.00, SD=1.04, p=1.0).
Ethical and public health considerations. Participants agreed that the simulation ‘should be incorporated into medical and caregiver training programs’ (M=4.57, SD=0.51, p<.0023) and ‘could help reduce disparities in delirium care and education’ (M=4.39, SD=0.50, p<.0023). ‘There are ethical concerns regarding the emotional intensity of VR-based delirium simulations’ was below the midpoint, but not significant (M=2.30, SD=1.02, p=.003). ‘I have concerns about the effort / costs involved in building such a system vs. its benefits’ was neutral (M=2.57, SD=1.08, p=.066).
Future directions for research. Participants agreed with ‘future VR studies should explore how delirium symptoms evolve over time’ (M=4.13, SD=0.63, p<.0023) and ‘VR-based multi-user simulations could improve interdisciplinary teamwork’ (M=4.48, SD=0.67, p<.0023).
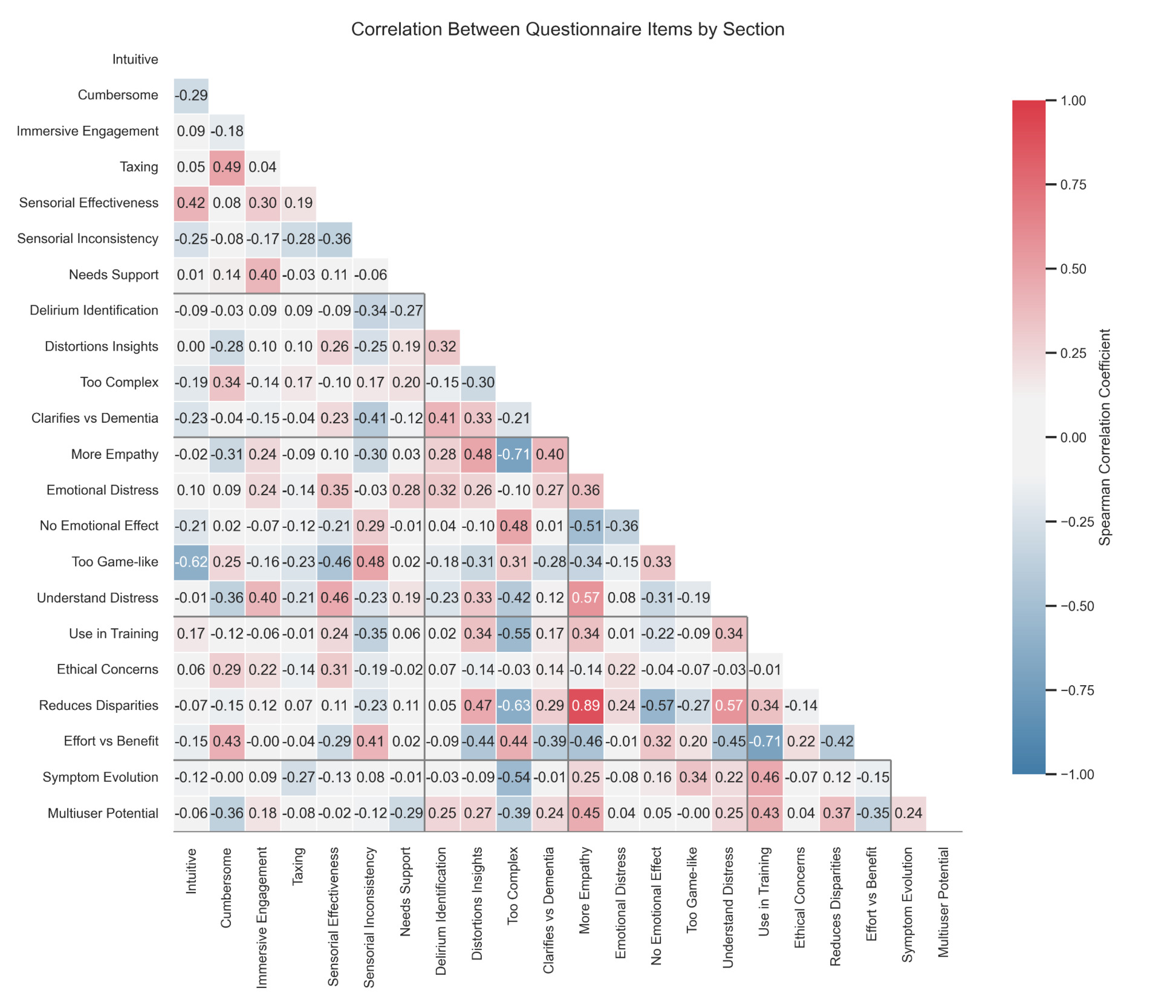
Inter-item correlations. Exploratory Spearman correlations (Figure 2) showed a few patterns in participant responses. Participants who reported an empathy increase also tended to report higher understanding of delirium: The reported increase in empathy correlated both with the understanding delirium patients’ emotional distress (ρ=.57) and cognitive distortions (ρ=.48); understanding delirium patients’ emotional distress and their cognitive distortions also correlated with each other (ρ=.35). Reporting increased empathy was also positively correlated with the belief that the simulation could reduce disparities in care (ρ=.47) and should be used in training (ρ=.34), and was negatively correlated with ‘viewing the experience of delirium patients in VR did not touch me’ (ρ=−.51).
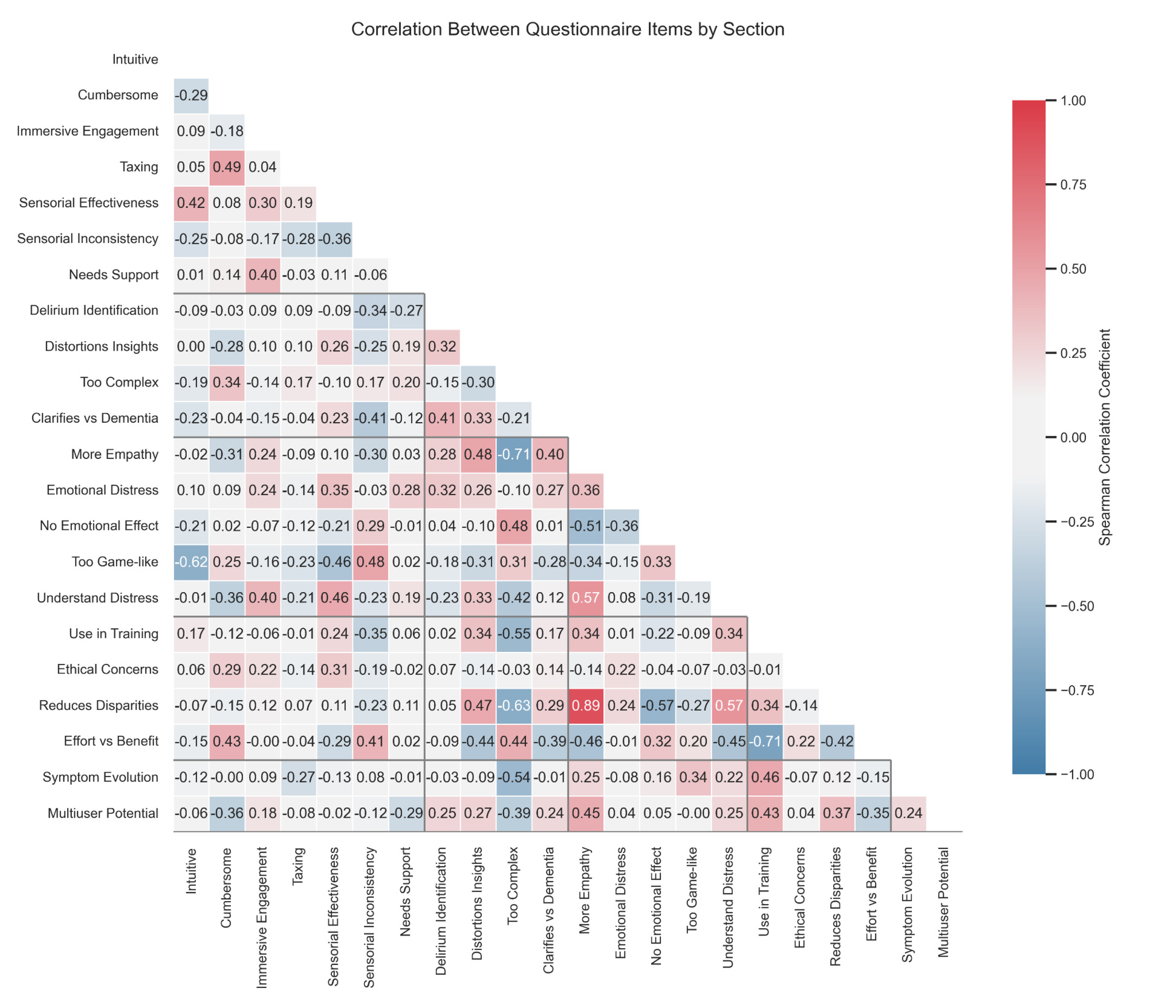
In contrast, participants who found the simulation less user-friendly, rating it as ‘cumbersome’, ‘taxing’, or ‘unnecessarily complex’, did not report higher understanding: Finding the VR simulation ‘unnecessarily complex’ negatively correlated with the understanding of delirium patients’ emotional distress (ρ=−.42). Finding it ‘cumbersome’ was correlated with finding it ‘taxing’ (ρ=.49) and finding the simulations’ sensory effects effective (ρ=.42), suggesting some appreciation of sensory realism despite cognitive load. However, these usability concerns did not correlate strongly (|ρ| ≥ .40) with endorsement (using it in training, its potential to reduce disparities and multi-user applications).
Qualitative results (Open-ended items)
21 participants responded to the question about whether ‘AI and adaptive/personalized VR could improve the realism and effectiveness of this training’. Many mentioned that personalization could increase realism and make the simulation more immersive (“By interacting with individual patients based on their own needs, fears and experiences, one could certainly enhance the experience. An AI algorithm could explore these personal traits.”). Enhancements in sensory immersion and interactivity were also recommended. 22 participants responded to the question about whether this simulation could be used for ‘early delirium diagnosis in clinical settings’. The most frequent response was that awareness could help diagnoses, but that the simulation is not a diagnostic tool per se (“To raise awareness of delirium and make people consider it as a differential diagnosis, help people to have more empathy for delirious patients”). 20 participants responded to the question about whether the simulation could improve ‘doctor-patient communication and bedside manner’. Most highlighted that VR could increase empathy by helping clinicians ‘see how patients might react’ and ‘have a better idea of what patients experience’. All 23 participants responded to the question about whether they would ‘recommend this simulation for patient or caregiver education’. The majority said they would recommend the simulation, often noting that it was simple and effective for caregivers to better understand patients’ confusion (‘because an experience is more memorable than a lecture’) and that it would benefit from more realism.
Finally, 19 participants gave suggestions on future research directions. Ideas included adding the interaction with family members, multi-sensorial experiences, and more scenarios and patient-doctors interactions. Several comments suggested developing more interactive and realistic scenarios adapted to different patients’ feedback. 18 participants responded to the question about new features or improvements for future VR simulations. Frequent suggestions were increasing realism (e.g., graphics, movement, smell), making the simulation less game-like, and expanding interaction possibilities.
Discussion
This pilot study adds to a growing body of research supporting the use of VR to foster empathy and clinical insight in health education. Participants reported increased empathy and greater insight into patients’ cognitive and emotional disturbances, consistent with prior work on VR-supported perspective-taking and engagement in clinical training.12,13 The correlation between reported empathy increase and improved understanding aligns with evidence that affect can support learning.32,33 Lasting learning outcomes can be achieved through the use of stories (referred to as narrative medicine34), which arguably is most beneficial to under-served communities, e.g., those with low literacy or cognitive impairment. Furthermore, if the realism levels are carefully crafted, there is evidence in prior work in other contexts that virtual environments can offer memorable experiences optimized for cognitive load concerns.35,36 Confirming the need for such optimization, in our pilot study, usability mattered: While usability ratings were overall positive, participants who perceived higher complexity or burden tended to report lower empathy and insight, highlighting the need to design emotionally powerful but technically accessible VR experiences. Qualitative responses emphasized the value of simulating the patient perspective and recommended further personalization, increased sensory realism, and inclusion of varied delirium presentations. Taken together, these findings from our pilot study provide early evidence that a concise, qualitatively grounded VR simulation of delirium is both feasible and valued by learners (not just experienced practitioners5,23), offering a strong foundation for scaled, patient-centred training. Some limitations need to be acknowledged. We used a study-specific, adapted questionnaire rather than validated scales; the small convenience sample of students, shared testing space, and reliance on immediate self-report limit generalizability. Notably, while reported empathy and insight increased, differentiation between delirium and dementia remained near neutral, suggesting that empathy-oriented VR may need to be complemented with targeted diagnostic training.
Future work following this pilot study should enroll clinically active learners, compare VR with active pedagogical controls, and incorporate behavioral outcomes (e.g., screening frequency/accuracy, recognition time, and communication quality). Testing adaptive (e.g., personalized depth of field simulation and motion control against cybersickness), interactive, and multi-user/team-based designs, as well as automated approaches to VR content creation to improve scalability, and comparative studies to alternative versions e.g., smartphone-based augmented reality (AR) versions are also envisioned. With these refinements, VR can complement conventional education by conveying the subjective experience of delirium while supporting practice-relevant learning.
Acknowledgements
We are grateful for our colleagues and students who joined us in the data collection efforts; and the event hosts, Dr. Sandra Bastelberger, Clara Lampe, and Nico Zobrist, for facilitating participant recruitment, as well as the use of the venue by the University of Zurich. We are thankful to the Swiss Study Foundation (Dr. Sandra Bastelberger) for having organized the educational event.
Author Contributions
Laura Fontanesi: Investigation; Formal analysis; Writing – original draft; Writing – review & editing; Visualization.
Arzu Çöltekin: Conceptualization; Methodology; Resources; Writing – review & editing; Supervision; Project administration; Funding acquisition.
Thomas Kunz: Conceptualization; Software; Investigation; Resources; Writing – review & editing.
Sandro Arrigoni: Software; Investigation.
Mathias Schlögl: Conceptualization; Resources; Writing – review & editing; Supervision; Funding acquisition.
Steven Bourke: Writing – review & editing.
Alasdair MacLullich: Writing – review & editing.
Rasita Vinay: Writing – review & editing.
Tobias Kowtasch: Writing – review & editing.
Nico Zobrist: Writing – review & editing.
Clara Lampe: Writing – review & editing.
Martina Schöpf: Writing – review & editing.
Vincenza Frisardi: Writing – review & editing.
Funding sources
The study was partially funded by Swiss Innovation Agency Innosuisse (project number: 39337.1 IP-ICT) for the members of the FHNW, as well as Draeger Schweiz AG and Clinic Barmelweid resources.
Declaration of Interests
RV and TK are affiliated with the Centre for Digital Health Interventions (CDHI), a joint initiative of the Institute for Implementation Science in Health Care, University of Zurich, the Department of Management, Technology, and Economics at ETH Zurich, and the Institute of Technology Management and School of Medicine at the University of St Gallen. CDHI is funded in part by the Swiss health insurer CSS, the Austrian health care provider (and corporate start-up of UNIQA) Mavie Next, and the Swiss investor MTIP. TK was also a co-founder of Pathmate Technologies, a university spin-off company that creates and delivers digital clinical pathways. However, neither CSS, Mavie Next, Pathmate Technologies nor MTIP were involved in this study. Furthermore, TK has neither shares of Pathmate Technologies nor any formal role in the company. NJZ receives a scholarship from the Swiss Study Foundation, funded by the Werner Siemens Foundation for the academic year 25/26. SB is the owner and founder of PersonalPulse. SB is a fellow of EUPATI foundation. CJL receives a scholarship from the German Academic Scholarship Foundation. All other authors declare no competing interests.