INTRODUCTION
Delirium is a change in mental status that can cause acute cognitive changes that fluctuate with time. It is an underrecognized problem in the medical setting that contributes to poor patient outcomes.1 Delirium occurs in all hospital units; however, the intensive care unit (ICU) carries the highest number of patients experiencing delirium. Decades of studies have illustrated the prevalence of ICU delirium affecting 11%-87% of ICU patients worldwide.2 Patients who experience ICU delirium have increased hospital days, more ventilator hours, higher healthcare costs, longer rehabilitation times, and an increased mortality rate than those who do not experience ICU delirium.3
The ICUs at an urban teaching hospital in the Midwest United States relied on the delirium subsection of the Society of Critical Care Medicine’s ICU Liberation Bundle (ABCDEF)4 to address the assessment, prevention, and management of ICU delirium. The delirium section of this bundle states that the nurse will perform the Confusion Assessment Method for ICU (CAM-ICU) scale once per shift and treat the patient’s pain.4 This bundle’s directives ensure patients are screened for ICU delirium. However, hospital ICUs had not previously educated nurses regarding delirium or ensured competent CAM-ICU assessments.
This quality improvement project aimed to a set of evidence-based delirium prevention strategies by creating a nurse-led Early Delirium Intervention (EDI) protocol for the neuroscience ICU (NSICU). The project built upon current evidence-based practices and delirium prevention research to mitigate the development of ICU delirium by applying the principles to patients admitted to a neuroscience ICU.5–8 The EDI protocol provides a list of delirium prevention strategies that should be implemented for every patient. It then guides ICU nurses through performing a delirium assessment using the CAM-ICU and responding to the result. This project’s measurable outcomes included (a) describing the fidelity of the EDI protocol, (b) examining the effect of the EDI protocol on NSICU patient outcomes, and (c) comparing NSICU nurses’ pre- and post-intervention knowledge and comfort with the CAM-ICU.
METHODS
Design
The hospital’s institutional review board determined that the project satisfied the requirements of a quality improvement project. This project utilized the Reach, Effectiveness, Adoption, Implementation, and Maintenance (RE-AIM) framework to develop and implement sustainable interventions to combat ICU delirium.9 The SQUIRE guidelines guided the project’s methodology and data reporting.10
Setting and Participants
This project was implemented in a 718-bed academic medical center’s 20-bed NSICU. The sample included all adult NSICU patients, regardless of hospital length of stay before project implementation. Intubated patients in the sample had orders to maintain their Richmond Agitation Sedation Scale (RASS) > -3, as the neurosurgery team’s orders for those with a RASS ≤ -3 were paired with a “no stimulation” order. Minors, age 18 and younger, and those with a RASS ≤ -3 were excluded from data collection.
Early Delirium Intervention Protocol
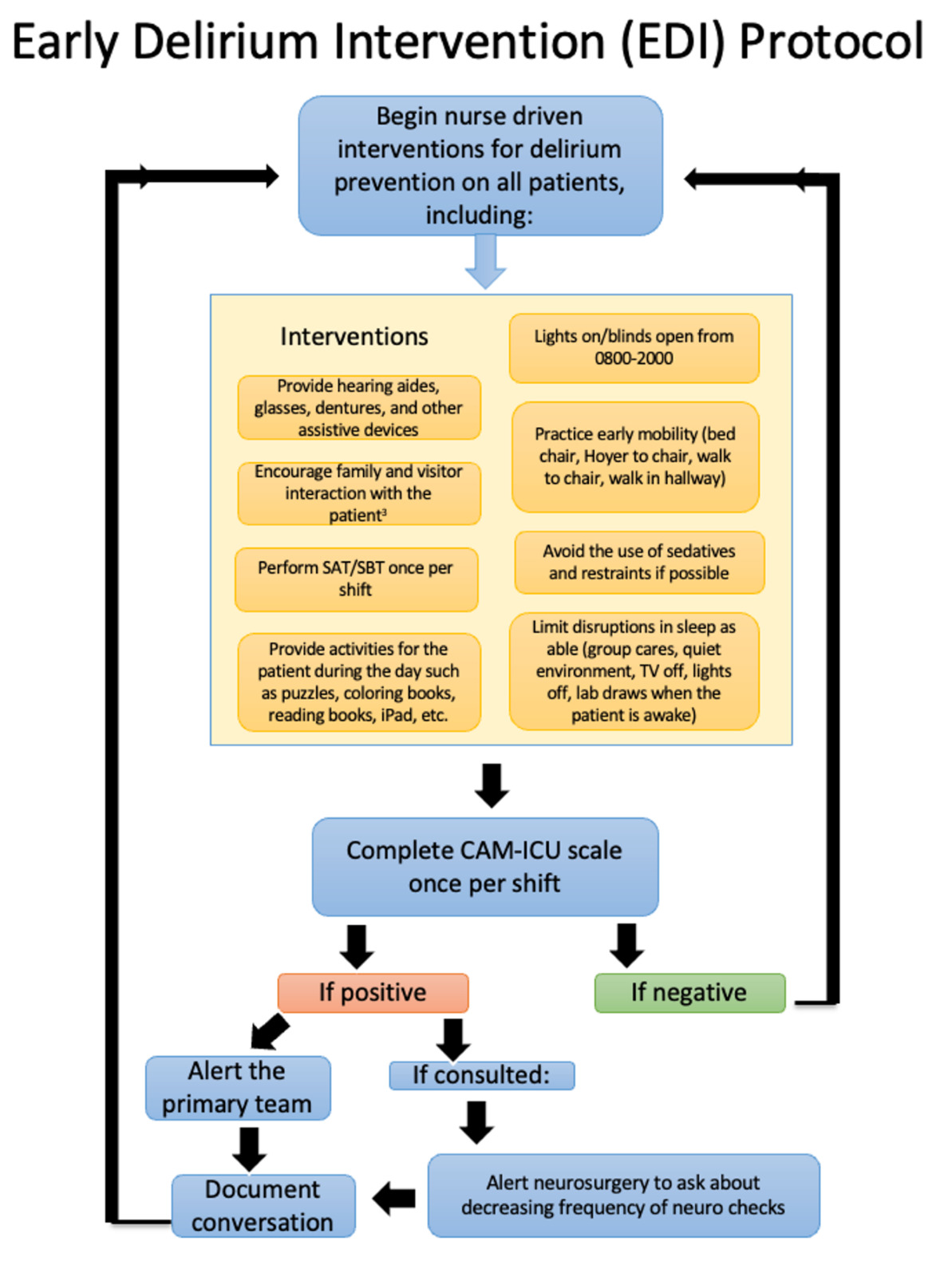
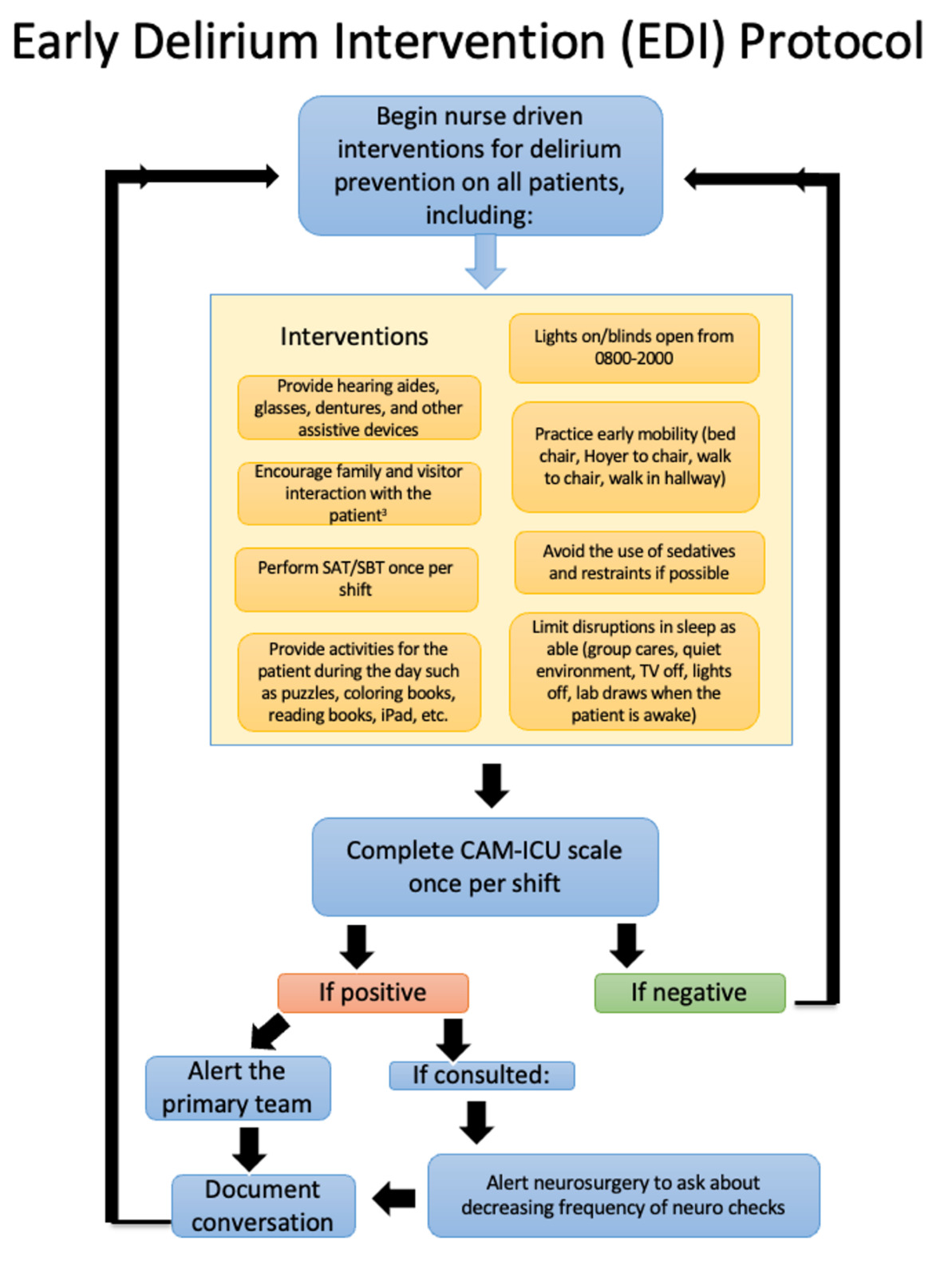
The EDI protocol (see Figure 1) was created using current evidence to ensure the best patient outcomes.4,7,8,11–14 The EDI protocol directed the initiation of nurse-driven methods for preventing delirium, including the following daytime interventions: (a) keeping lights on, (b) blinds open, (c) televisions on to channels that may maintain orientation such as news programs, (d) orienting the patient with each interaction, (e) ensuring use of hearing aids, glasses, and dentures, and (f) providing cognitive stimulation activities such as puzzles, crosswords, coloring books, and fidget toys.15 Nighttime interventions called for keeping lights off, the door closed, televisions off, and a quiet environment free of interruption. The protocol prompted nurses to complete the CAM-ICU on all patients once every 12 hours, triggering a provider notification for positive CAM-ICU scores.
Intervention
The EDI protocol was implemented in the NSICU for 8-weeks. Target outcomes were compared to an 8-week pre-implementation baseline.
Nursing Education
Education on the nurse-led EDI protocol was provided to nurses daily during the week preceding the implementation of the EDI protocol. Nursing education included a live presentation with visual aids to illustrate the importance of delirium screening, including a review of the adverse outcomes associated with ICU delirium. A delirium screening competency was created for the NSICU nurses, which began with an exemplary demonstration of an experienced NSICU nurse performing a CAM-ICU on a simulated patient with a negative and positive screening result. The nurses received further reinforcement of the importance of prompt provider notification of a positive CAM-ICU screening. After each educational session, the nurses were provided time to practice the CAM-ICU and ask questions. The EDI protocol was posted in the staff break room and at the nurses’ stations for ongoing reference. A follow-up electronic communication to the nursing staff highlighted expectations associated with the EDI protocol.
Data Collection
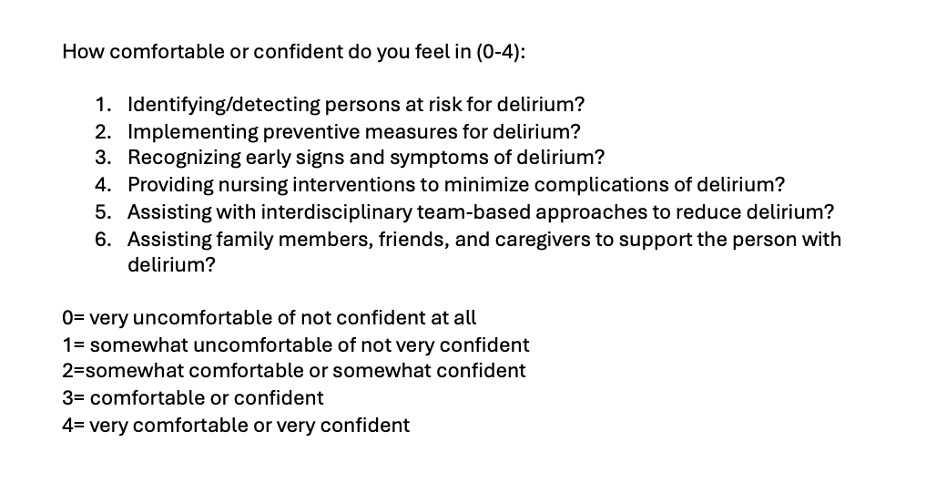
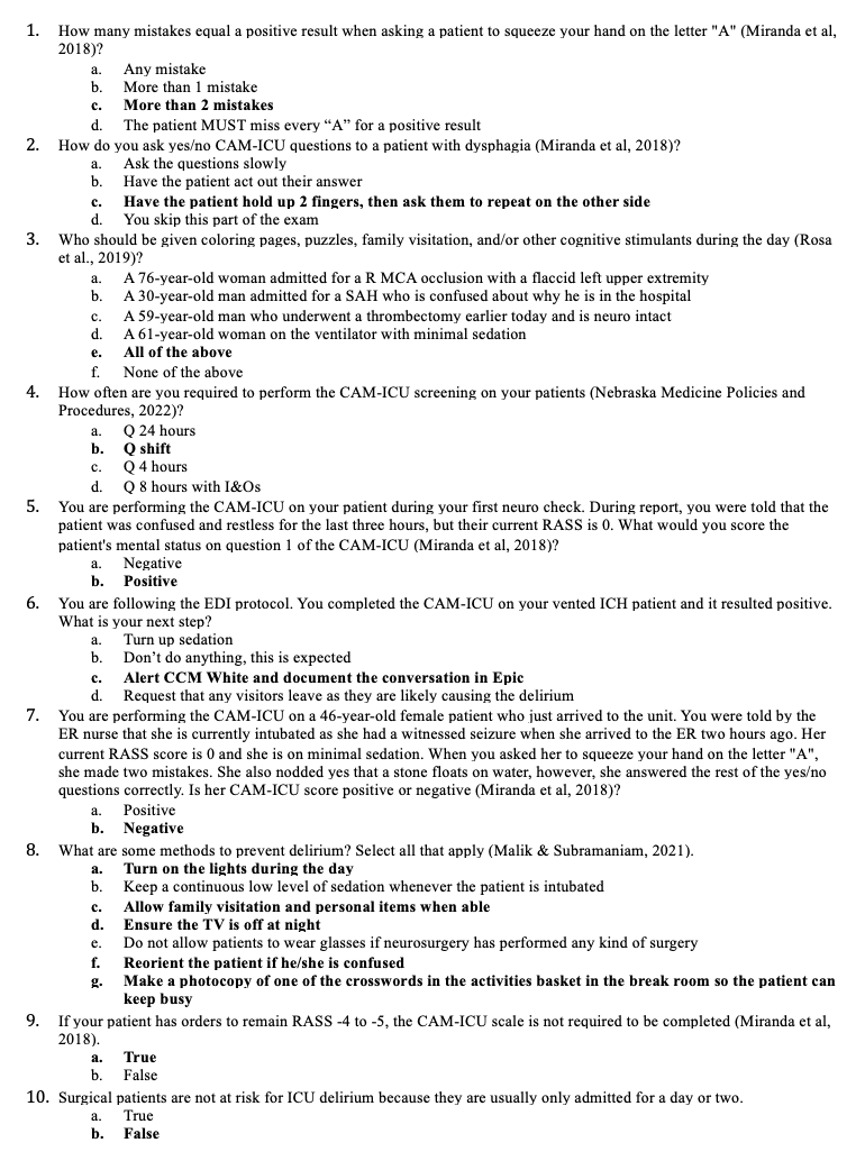
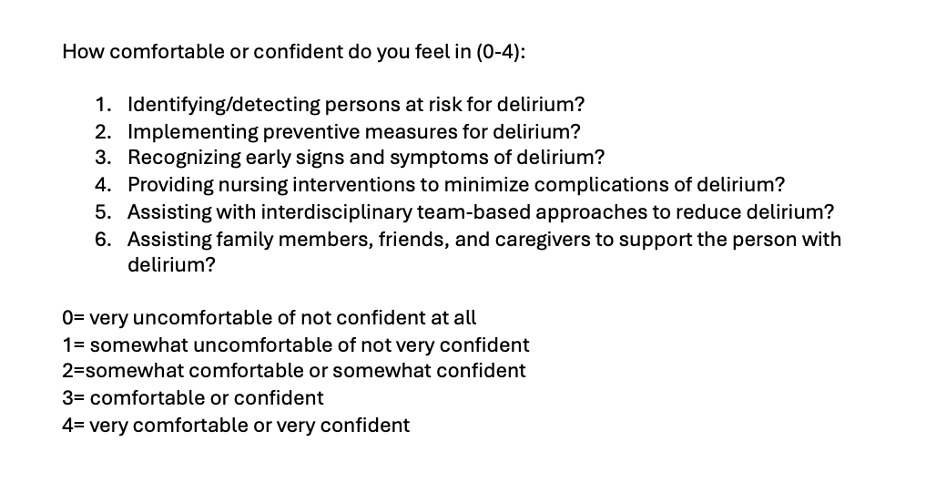
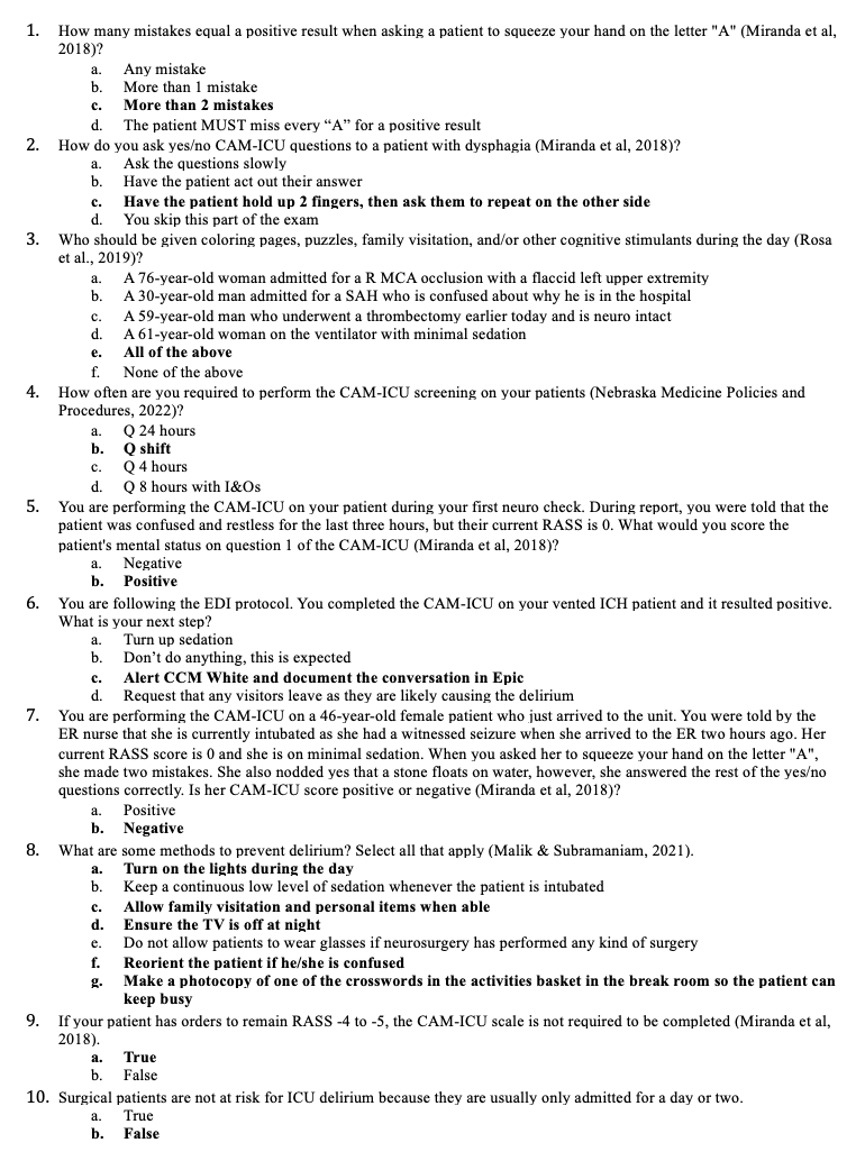
Before receiving education on the EDI protocol, NSICU nurses completed the American Nurses Association’s Delirium Survey to assess their comfort in recognizing ICU delirium (see Figure 2).16 At the same time, a Delirium Knowledge Assessment captured the NSICU nurses’ knowledge of current evidence and hospital policies on delirium (see Figure 3). After receiving education, the nurses repeated the two surveys to assess for changes in their knowledge of and comfort with the CAM-ICU.
Lead nurses on each shift audited all NSICU hospital rooms during the pre-and post-implementation period for evidence of the EDI-protocol-driven delirium prevention measures. During the eight weeks preceding and eight weeks following the implementation of the EDI protocol, the following information was extracted from the electronic medical record of patients meeting project inclusion criteria: (a) CAM-ICU screening documentation, (b) total ventilator hours per patient, (c) ICU length of stay per patient, (d) provider notification of positive CAM-ICU results, and (e) new prescriptions for Seroquel (quetiapine).
Data Analysis
The six Likert-scale items for rating the NSICU nurses’ perceptions of comfort with the CAM-ICU were averaged. We used a Kruskal-Wallis rank sum test to compare responses in the pre-implementation phase to the post-implementation phase. To assess staff competency with the CAM-ICU, we used a between-subjects t-test to compare scores on the 10-question knowledge assessment. A between-subjects test was selected because staff identity was not collected to preserve anonymity.
Generalized linear mixed models were used to test whether the EDI protocol improved CAM-ICU checklist scores, nesting pre versus post between individual ICU rooms. CAM-ICU scores were averaged within a day and fit to a Gaussian distribution. If significant, individual CAM-ICU items were analyzed separately and fit into a binomial distribution.
RESULTS
Sample Demographics
Of the 50 NSICU nurses eligible for EDI protocol education, 70% (n = 35) received face-to-face teaching, and all received electronic communication of the EDI protocol expectations.
The pre-and post-intervention patient samples were similar in size (pre: n = 185 vs. post: n = 190) and mean age (pre: M = 62.04 years vs. post: M = 60.3 years). However, there was a disparity in gender, with a 58.3% male population in the pre-intervention group and 44.7% in the post-intervention group (see Table 1).
Nurse Education
The NSICU nurses’ ANA Delirium survey results increased from pre-implementation (median = 3) to post-implementation (median = 4) (K-W χ2 = 14.864, p = 0.0001156). Delirium Knowledge Assessment scores increased from pre-implementation (M = 74.4%) to post-implementation (M = 89.1%) (t(47) = 4.02361 p = 0.000206).
Delirium Prevention Measures
The nursing staff completed a mean of 57% of the evidence-based delirium prevention measures daily during the project implementation interval, compared to 49.7% during the pre-implementation interval. Adherence to the delirium prevention measures of keeping the lights on during the day (χ2 = 6.3396, df=1, p = 0.01181), television on during the day (χ2 = 5.099, df=1, p = 0.02394), and cognitively stimulating activities (χ2 = 16.043, df=1, p <0.001) increased during the post-implementation phase, as compared to the pre-implementation phase. Completion of checklist items was similar between the pre-implementation (89.8%) and post-implementation (93.0%) phases.
Delirium Screening Documentation
Nurse documentation of CAM-ICU screenings improved during the day shift hours in the project’s post-implementation phase compared to the pre-implementation phase (F(1,25.193) = 9.9765, p = 0.004088). The night shift CAM-ICU documentation performance was unchanged from the pre- to post-implementation phases (F(1,28.122) = 1.5462, p = 0.224).
Provider Notification of Delirium
The nursing staff documented provider notification in 0.11% of positive CAM-ICU results in the pre-intervention period (n=2), which was stable compared to 0.03% in the post-intervention group (n=2).
Patient Outcomes
The ICU length of stay decreased from 4.41 days pre-implementation to 3.15 days post-implementation (p=0.0666). The ventilator hours decreased from 100.83 hours pre-implementation to 68.22 hours post-implementation (p=0.1315). The proportion of patients in the sample with a new Seroquel (quetiapine) prescription increased from 1.62% to 5.79.
Discussion
Day-shift completion of the CAM-ICU scale and fidelity to the EDI protocol improved significantly during this project, indicating an enhanced overall adoption of the EDI Protocol among the day-shift nursing staff. Night-shift CAM-ICU completion rates were unchanged. Delirium prevention measures require consistent implementation, and this project’s outcomes highlight the importance of increased engagement with night-shift nurses to identify barriers to delirium prevention and screening measures. Night shift overall participation could be improved by increasing the presence of the nurse manager, supervisor, or educator at night to encourage adherence to the EDI protocol, including multidisciplinary teams such as phlebotomy to draw labs in daylight hours, or requesting that providers order extended intervals of quiet time at night to promote sleep.
One of the focuses of the EDI Protocol was early provider notification of a positive CAM-ICU screening. Nevertheless, nurse documentation of provider notification was poor in the pre- and post-implementation periods. Although the rate of provider notification documented for positive delirium scores was low, it is possible that nurses did notify providers without documentation, and particular providers preferred medication for delirium treatment.
The identified increase in the use of Seroquel could be due to provider preference, more patients being admitted with Seroquel as a home medication, increased need for antipsychotic medication in patients with acute neurological conditions, or reasons not captured through data collection. The increased use of Seroquel in the NSICU population during the intervention period is concerning, as there is a lack of solid data to suggest that the use of antipsychotics improves the outcomes of patients with delirium.17
Plans within this facility are to implement the EDI protocol in the hospital’s five ICUs
and include specific one-on-one education with all nurses and begin EDI education with nursing assistants when they begin employment in one of the ICUs. Yearly in-person competencies allow space for continued CAM-ICU and delirium prevention education. In replicating this project, the authors recommend dedicating data collectors and not relying on nursing staff to collect data. Education for nursing assistants and other multidisciplinary specialties who spend significant time at patients’ bedsides would increase adherence to delirium prevention measures. Lastly, the authors recommend educating ordering providers about the expectations of the EDI protocol and ways they can support nursing, such as limiting medications that affect mental status, following Beers Criteria in older adults, and transferring patients out of ICU as soon as they are medically stable to facilitate better outcomes.18
Strengths and Limitations
Implementing the EDI Protocol provided nurses with a robust knowledge of delirium and a set of interventions they could implement on patients to prevent the development of delirium. The methods of delivering nursing education on delirium prevention and early recognition were a strength of this project. Along with the education presented, nurses observed and practiced CAM-ICU assessments, which yielded a statistically significant improvement in nurses’ knowledge of delirium and comfort with the CAM-ICU. Nurses maintain a consistent presence at the bedside, ideal for preventing and ensuring prompt recognition of ICU delirium. The brisk improvement in nurses’ knowledge and comfort scores following the educational intervention exemplifies the importance of in-person nursing education on delirium, including the opportunity to ask questions and practice delirium assessment skills.
This project’s outcomes were limited by a 70% nurse education rate, as travel nurses, new hires, and nurses who floated to the NSICU from other units did not receive in-person education on the EDI Protocol. All NSICU nurses received a follow-up email with a summary of educational points, but there was no method to ensure that the nurses read and understood the information. Gaps in the reach of nursing education may have adversely impacted nurse adoption and the protocol’s fidelity. Additionally, the lack of consistency in charge nurse audits of the delirium prevention measures may have adversely affected the reporting and reinforcement of the delirium prevention measures delineated in the EDI Protocol.
CONCLUSION
This quality improvement project demonstrated the feasibility of nurse-led delirium prevention measures in the ICU. The project’s educational intervention included demonstrating the CAM-ICU assessment and dedicated time for nurses to practice this assessment skill. Project outcomes showed a statistically significant improvement in CAM-ICU documentation, nurses’ knowledge of delirium, and nurses’ comfort with the CAM-ICU assessment. Implementing nurse-driven delirium prevention and early identification strategies empowers nurses to play a crucial role in promoting positive outcomes for critically ill patients.
Author Contributions
Megan Schoepke, DNP, AGACNP-BC, was responsible for conceptualization, investigation, and writing the original draft.
Theresa A. Jizba, DNP, AGACNP-BC, ACHPN, was responsible for supervision, writing, review, and editing.
Jack Taylor, PhD was responsible for data curation and formal analysis.
Disclosure/Conflict of Interest
The authors have no financial relationships relevant to this article and no conflicts of interest to disclose.
Funding Sources
This research received no specific grant from public, commercial, or not-for-profit funding agencies.
Institutional Review Board Approval
The project was reviewed by the University of Nebraska Medical Center and the Creighton University IRB (submission #2004188-01). Both IRBs determined that the project satisfied the requirements of a quality improvement project and did not require further IRB oversight.