ABBREVIATIONS
CAM, Confusion Assessment Method
CAM-ICU, Confusion Assessment Method for the Intensive Care Unit
ICU, intensive care unit
IQR, interquartile range
NIA, National Institute on Aging
RASS, Richmond Agitation-Sedation Scale
INTRODUCTION
Delirium, an acute change in attention or cognition that typically occurs after a critical illness or major surgery, occurs in an estimated 10-47% of liver recipients after transplant surgery.1–10 In recent years, studies in critically ill populations found that delirium was associated with inferior patient outcomes, including longer hospital length of stay and higher risk of in-hospital mortality.11 This has prompted renewed interest in delirium in liver transplant recipients, a population at high risk for this complication.
At many centers, including our own, routine delirium assessments of liver transplant recipients have historically been limited to the intensive care unit (ICU). However, decreases in ICU length of stay from 5-6 days to 2-3 days over the past two decades have truncated the period of post-transplant monitoring for delirium.12–14 Work from our group that is currently in press showed that 11% of recipients overall and 30% of recipients identified as having delirium in the ICU were delirious on the day of their transfer out of the ICU to the surgical floor15; this suggests that delirium likely continues – and may occur de novo – for some recipients after leaving the ICU.
Therefore, we performed a longitudinal cohort study of liver transplant recipients to assess for delirium in both the intensive care unit and on the surgical floor.
METHODS
Study population
We approached all adult (≥18 years old) liver recipients at the Johns Hopkins Hospital from September 6, 2022 to May 31, 2024 about participation in our study. When possible, recipients were approached after a donor offer had been accepted but prior to their transplant surgery. Participants who could not be approached prior to transplant due to logistical constraints (e.g. short time frame between offer acceptance and surgery) or patient preference were approached and/or enrolled after transplant surgery. Given that many potential participants lacked capacity immediately post-transplant, when necessary, consent discussions were held with a potential participants’ family. When consent was obtained from someone beside the potential participant, consent to continue participating in the study was obtained again from the participant when they regained capacity. This study was approved by the Johns Hopkins Institutional Review Board (IRB00321352) and written consent was obtained for all participants.
Delirium assessment
Delirium was assessed by study team members who had received group and on-on-one instruction in the administration of the instruments from a psychiatrist. Assessments were performed using two validated instruments at each interaction.
The first instrument administered was a version of the Confusion Assessment Method (CAM) instrument, either the CAM-ICU while participants were in the intensive care unit or the CAM short form while patients were on the surgical floor. Both the CAM-ICU and the CAM short form were created as bedside assessment tools for non-psychiatrists to assess for delirium in critically ill patients and non-critically ill patients, respectively.16,17 These assessments are valid for patients who have a Richmond Agitation-Sedation Scale (RASS) score of >-4 (i.e. no coma or stupor). A “positive” score on the CAM-ICU or the CAM short form indicates delirium is present and occurs if a patient demonstrated an acute change or fluctuating course of mental status within the last 24 hours, inattention, and at least one of the following: altered level of consciousness (defined by RASS score) or disorganized thinking. No other cognitive tests were done prior to performing the CAM instrument.
The second instrument administered was the 4AT, which was used to assess participants at every interaction.18 This screening instrument is designed for rapid initial assessment of delirium in patients and covers 4 items beginning with ‘A’: alertness, Abbreviated Mental Test-4, attention, and acute change or fluctuating course of mental status.19 On the 4AT, a score of ≥4 suggesting possible delirium and a possible need for more detailed assessment. The 4AT can be used both in the intensive care unit (ICU) and on the surgical floor.
The CAM-ICU and CAM short form were selected because of the wide body of literature using these tools, as well as their previous use in liver transplant recipients. We chose to also use the 4AT because it could be used consistently across all assessments, whether the patient was in the intensive care unit or on the surgical floor.
Daily delirium assessments were performed before transplant and for the first 14 days after transplant or until discharge, whichever came first. Daily assessments were attempted by a study team member up to three times on a given day; assessment was deferred to prioritize patient care (e.g. working with physical therapy) or due to participant preference.
Data abstraction
We abstracted participants’ demographic characteristics (age, sex, race, ethnicity, liver disease etiology), clinical characteristics (liver disease etiology, history of hepatic encephalopathy), transplant characteristics (type of transplant donor) from the electronic medical record.
Statistical analysis
Participant characteristics were compared by whether a recipient experienced delirium during their transplant hospitalization using Chi-squared and rank-sum tests for categorical and continuous variables, respectively. Categorical variables are reported as number (percent), while continuous variables are reported as median (interquartile range).
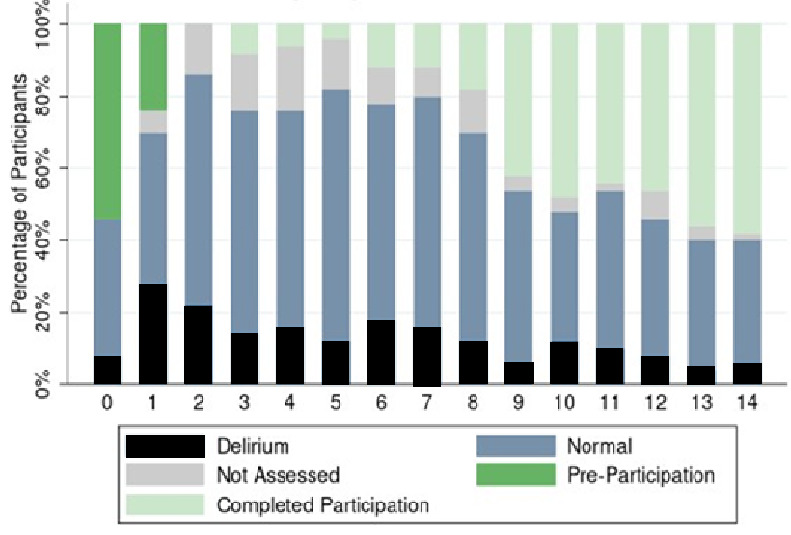
Delirium course was evaluated using descriptive statistics. Daily status (normal, delirium, or not assessed) was visualized for participants on each day post-transplant. Cumulative incidence of developing delirium was visualized. All analyses were performed using Stata 17.0/MP for Windows (College Station, Texas).
RESULTS
Study Population
Among the 50 participants, the median (interquartile range, IQR) age was 54 (46-63) years old, 66% were male, 82% were of White race, and 4% were of Hispanic ethnicity (Table 1). The highest level of educational achievement was high school for 20%, some college for 24%, a college degree for 30%, and post-graduate education for 26%. The most common liver disease etiology was alcohol-related liver disease (54%), and 54% had a history of hepatic encephalopathy. Organ donors were deceased for 76% of participants and living for 24% of participants. Of the 50 participants, 23 (46%) were assessed for delirium prior to transplant, of whom 4 (17%) screened positive for delirium prior to transplant surgery. While alcohol-related liver disease was more common among recipients who developed delirium than among those who did not, this difference was not statistically significant (62% vs. 43%, p=0.43). Otherwise, pre-transplant characteristics were statistically similar between recipients with and without post-transplant delirium (Table 1).
Delirium in the Intensive Care Unit
Of the 50 participants, 43 (86%) were assessed for delirium in the intensive care unit post-transplant (Figure 1). Among those assessed using the 4AT, 20/43 (47%) screened positive for delirium. Among those assessed using the CAM-ICU, 11/42 (26%) screened positive for delirium. All participants who screened positive for delirium on the CAM-ICU also screened positive for delirium on the 4AT. Therefore, overall, 20/43 (47%) of participants screened positive for delirium while in the intensive care unit.

Delirium on the Surgical Floor
Of the 50 participants, 49 (98%) were assessed for delirium on the surgical floor. Delirium was identified among 21/49 (43%) of participants assessed using the 4AT and 8/48 (17%) of participants assessed using the CAM-S. All participants who screened positive for delirium on the CAM-S also screened positive for delirium on the 4AT. Therefore, 21/49 (43%) of participants overall screened positive for delirium while on the surgical floor.
Delirium during the Transplant Hospitalization
Of the 50 participants, 29 (58%) screened positive for delirium during the transplant hospitalization. Of the participants identified as having delirium, 12 (41%) were captured as having delirium both in the ICU and on the surgical floor, 8 (28%) were captured as only having delirium in the ICU. Additionally, 9 (31%) participants were captured as only having delirium on the surgical floor, although 5 of these participants had not been assessed in the ICU, typically due to the short length of their ICU stay [median (IQR) 2 (1-3) days).
Transplant Hospitalization Length of Stay
Overall, the median (IQR) length of stay was 2 (2-4) days in the ICU and 14 (8-20) days in the hospital. Compared to recipients without post-transplant delirium, recipients with delirium had similar ICU length of stay [3 (2-5) vs. 2 (1-3) days, p=0.24] but significantly longer transplant hospitalization length of stay [16 (13-20) vs. 8 (8-13), p=0.004].
CONCLUSION
In this single-center longitudinal prospective cohort study of delirium in liver transplant recipients, 58% of recipients experienced delirium during the first 14 days of their transplant hospitalization, including in 47% of participants in ICU and 43% on the floor. Notably, 9 participants (18%) were captured as only having delirium on the floor, suggesting a need to monitor for incidence delirium occurring on the surgical floor in this population.
We observed a high incidence of delirium overall, in the intensive care unit, and on the surgical floor. Notably, while our estimate of post-liver transplant delirium in the ICU (47%) is within the range of 10-47% previously published prevalence estimates,1–10 our estimate of overall delirium prevalence (58%) exceeds previous estimates, likely because of the additional recipients experiencing delirium on the surgical floor that were identified by our longitudinal assessments. Additionally, we found a difference in the incidence of delirium when using the CAM instruments versus the 4AT. In both the intensive care unit and on the surgical floor, the 4AT detected a higher prevalence of delirium than the CAM instruments. Prior studies in non-transplant populations have had mixed results about the sensitivity of the 4AT versus CAM, with one finding greater sensitivity20 but a meta-analysis finding similar sensitivity 4AT and CAM.21 Another study noted that in real-world practice, the CAM may show positive scores below the expected rates in the population concerned, suggesting it may offer a conservative estimate of delirium prevalence.22 These differences underscore both the importance of understanding the strengths and weaknesses of each screening tool, as well as the role of formal psychiatric or neurologic evaluation of recipients when their mental status is unclear.
Notably, delirium was more common among recipients with a history of hepatic encephalopathy (66% vs. 38%, p=0.06) and those who had pre-transplant delirium (29% vs. 0%, p=0.08), though neither of these differences reached statistical significance. This was not surprising, given that there are many similarities between hepatic encephalopathy and delirium, and they can be difficult to distinguish clinically. In fact, they may be overlapping syndromes, with hepatic encephalopathy having a clearer etiology (liver dysfunction) and delirium often being multifactorial. Hepatic encephalopathy should improve after the transplant allograft begins to function, making it more likely that any observed changes in mental status are due to delirium the further one gets from surgery (assuming good allograft function). However, we find it both difficult and of limited utility to distinguish between delirium and hepatic encephalopathy in the perioperative period, especially given that the preventive care used to reduce and address delirium, such as the ABCDEF bundle, is likely beneficial for altered mental status due to either condition.23
One of our most important findings was the high prevalence of delirium on the surgical floor, including cases of incident post-transplant delirium on the surgical floor. Frequently, as at our center, there is not routine delirium assessment after recipients leave the ICU. This makes the presence of delirium on the surgical floor an important issue, as prior studies have shown that delirium goes underrecognized without routine assessment.24,25 While the nursing ratio on the surgical floor are substantially different than in the intensive care unit, tools such as the 4AT or CAM short form can be administered in under two minutes, making them easy to incorporate into routine assessments.26 Our findings confirm that liver transplant recipients remain at high risk for experiencing delirium on the surgical floor and that ongoing assessment for delirium is warranted after transfer out of the ICU. We also found that some recipients remain delirium-free in the ICU but develop incident delirium on the surgical floor. Therefore, delirium prevention initiatives remain important even after the critical phase of the patients’ post-transplant care. Implementation of existing delirium prevention initiatives designed for the critical care setting (e.g. the ABCDEF bundle)27 and for abdominal surgery patients28 should be considered to reduce post-transplant delirium.
We recognize that there are limitations to our study, including a sample size of 50 recipients, which limited power to evaluate for differences between recipients with and without delirium. However, this number represents the number of transplants performed annually at an intermediate-volume liver transplant center in the United States,29 and we believe this population provides important insights into the delirium course of liver recipients after transplantation. Furthermore, each delirium tool has specific characteristics (eg length of time required for completion, instrument validation in the population to be screened, limitations in differentiating potentially relevant neurologic conditions from delirium) that providers should consider before selecting one to integrate into their clinical care.30 Additionally, we recognize that our study team was unable to assess each recipient every day of their transplant hospitalization, and that those recipients that were assessed were only assessed once per day. Furthermore, the median length of stay for recipients in whom we did not identify delirium post-transplant was significantly shorter than that of those in whom we did identify delirium (median 8 vs. 16 days, p=0.004), highlighting the limited period of time in which we were able to observe some recipients. While these are important limitations, they also suggest that our estimate of delirium prevalence is likely conservative. We encourage additional studies in larger cohorts, possibly with multiple assessments each day.
In conclusion, we found that liver transplant recipients were at high risk for delirium not only in the intensive care unit but also on the surgical floor, with an overall transplant hospitalization prevalence of post-transplant delirium of 58%. Given that over half of liver recipients experience delirium during the course of their hospitalization, further studies to characterize delirium and work on preventing delirium in this population are warranted to optimize care of liver transplant recipients. Additionally, we recommend that routine delirium assessments become standard of care not only in the intensive care unit but on the surgical floor for liver transplant recipients.
ACKNOWLEDGEMENTS
This work was supported by grant number F32AG067642 (PI: Ruck) from the National Institute on Aging (NIA). The analyses described here are the responsibility of the authors alone and do not necessarily reflect the views or policies of the Department of Health and Human Services, nor does mention of trade names, commercial products or organizations imply endorsement by the U.S. Government.
AUTHOR CONTRIBUTIONS
Jessica M. Ruck – conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, software, supervision, visualization, writing – original draft, writing – review & editing
Alexis A. Jefferis – data curation, writing – original draft, writing – review & editing
Mayan Teles – data curation, writing – review & editing
Aura Teles – data curation, writing – review & editing
Sherif M. Helmy – data curation, writing – review & editing
Andrew M. Cameron – writing – review & editing
Karin Neufeld – conceptualization, methodology, supervision, writing – review & editing
Esther Oh – supervision, writing – review & editing
Elizabeth A. King – conceptualization, methodology, project administration, resources, software, supervision, writing – review & editing
ETHICS STATEMENT
This study was approved by the Johns Hopkins Institutional Review Board (IRB00321352) and written consent was obtained for all participants. This research was conducted in compliance with the Declaration of Helsinki, and consent was obtained in adherence to the Belmont Report principles.
FUNDING
This work was supported by grant number F32AG067642 (PI: Ruck) from the National Institute on Aging (NIA).
DECLARATION OF INTERESTS
The authors of this manuscript have no conflicts of interest to disclose as described by Delirium.